

Corticosterone mediates electroacupuncture-produced anti-edema in a rat model of inflammation
- PMID: 17697336
- PMCID: PMC1976320
- DOI: 10.1186/1472-6882-7-27
Corticosterone mediates electroacupuncture-produced anti-edema in a rat model of inflammation
Abstract
Background: Electroacupuncture (EA) has been reported to produce anti-edema and anti-hyperalgesia effects on inflammatory disease. However, the mechanisms are not clear. The present study investigated the biochemical mechanisms of EA anti-inflammation in a rat model.
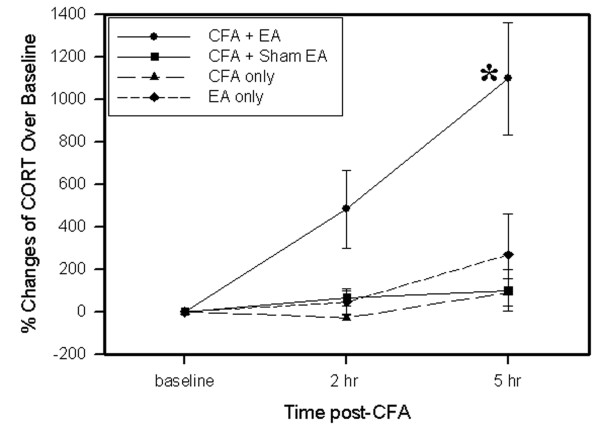
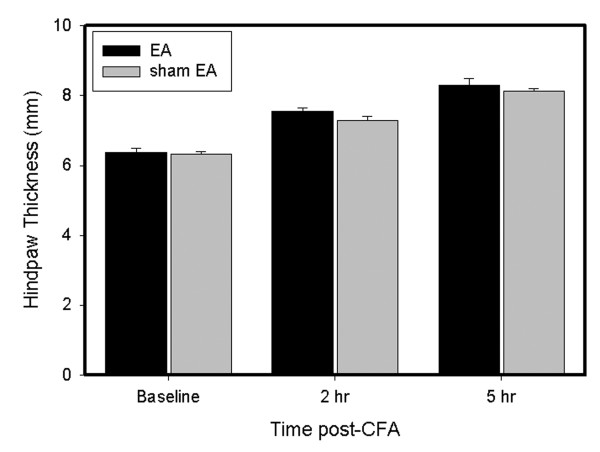
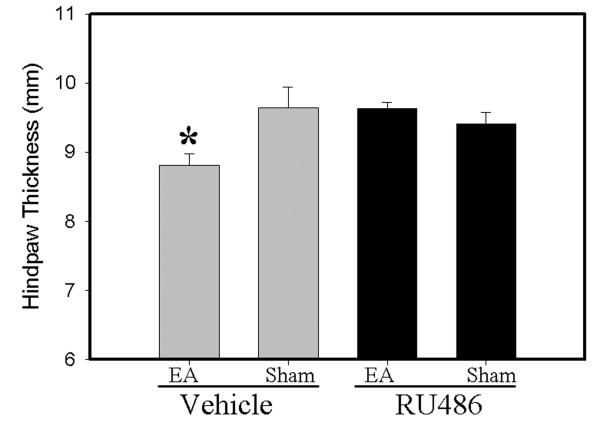
Methods: Three experiments were conducted on male Sprague-Dawley rats (n = 7-8/per group). Inflammation was induced by injecting complete Freund's adjuvant (CFA) subcutaneously into the plantar surface of one hind paw. Experiment 1 measured plasma corticosterone (CORT) levels to see if EA regulates CORT secretion. Experiment 2 studied the effects of the adrenal gland on the therapeutic actions of EA using adrenalectomy (ADX) rats. Experiment 3 determined whether a prototypical glucocorticoid receptor antagonist, RU486, affects EA anti-edema. EA treatment, 10 Hz at 3 mA and 0.1 ms pulse width, was given twice, for 20 min each, once immediately after CFA administration and again 2 h post-CFA. Plasma CORT levels, paw thickness, indicative of the intensity of inflammation, and paw withdrawal latency (PWL) were measured 2 h and 5 h after the CFA injection.
Results: EA significantly increased plasma corticosterone levels 2 h (5 folds) and 5 h (10 folds) after CFA administration compared to sham EA control, but EA alone in naive rats and CFA alone did not induce significant increases in corticosterone. Adrenalectomy blocked EA-produced anti-edema, but not EA anti-hyperalgesia. RU486 (15 mul, 15 mug/mul), a prototypical glucocorticoid receptor antagonist, also prevented EA anti-edema.
Conclusion: The data demonstrate that EA activates the adrenals to increase plasma corticosterone levels and suppress edema and suggest that EA effects differ in healthy subjects and in those with pathologies.
Figures

References
-
- Stiel D. Exploring the link between gastrointestinal complications and over-the-counter analgesics: current issues and considerations. American Journal of Therapeutics. 2000;7:91–98. - PubMed
-
- Davies NM, Jamali F. COX-2 selective inhibitors cardiac toxicity: getting to the heart of the matter. J Pharm Pharm Sci. 2004;7:332–336. - PubMed
-
- Cheng X. Chinese Acupuncture and Moxibustion. Beijing , Foreign Languages Press; 1999. p. 590.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
