

Management of insertional Achilles tendinopathy through a Cincinnati incision
- PMID: 17697370
- PMCID: PMC1976314
- DOI: 10.1186/1471-2474-8-82
Management of insertional Achilles tendinopathy through a Cincinnati incision
Abstract
Background: About 10% of patients not responding to 3-6 months of conservative management for insertional Achilles tendinopathy undergo surgery. Traditionally, surgery of the Achilles tendon is performed through longitudinal extensile incisions. Such surgery is prone to the complications of wound healing, wound breakdown and iatrogenic nerve injury.
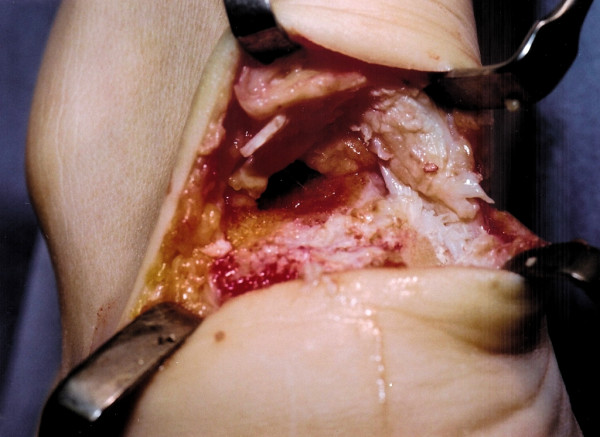
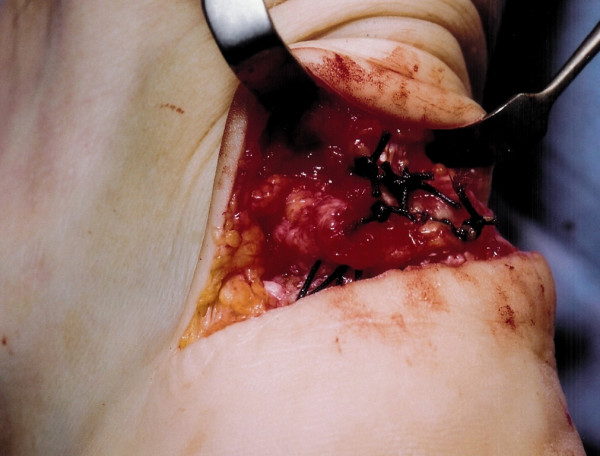
Methods: We describe our current method of exposure of the Achilles tendon insertion and debridement of the peritendinous and tendon tissue with osteotomy of the calcaneum through a transverse skin incision at the level of the Achilles insertion.
Results: This method has been used since 2002 on over 40 patients for exposure of the Achilles tendon insertion and the distal Achilles tendon.
Conclusion: The Cincinnati incision allows adequate exposure, has minimal risk of symptomatic iatrogenic nerve injury, and has minimal problems related to the scar.
Figures







References
-
- Clain MR, Baxter DE. Achilles tendonitis. Foot Ankle. 1992;13:482–487. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
