

Value and limitations of contrast-enhanced MR angiography in spinal arteriovenous malformations and dural arteriovenous fistulas
- PMID: 17698524
- PMCID: PMC7977648
- DOI: 10.3174/ajnr.A0612
Value and limitations of contrast-enhanced MR angiography in spinal arteriovenous malformations and dural arteriovenous fistulas
Abstract
Background and purpose: The purpose of this work was to study the validity of MR angiography (MRA) for identification of spinal arteriovenous (AV) abnormalities.
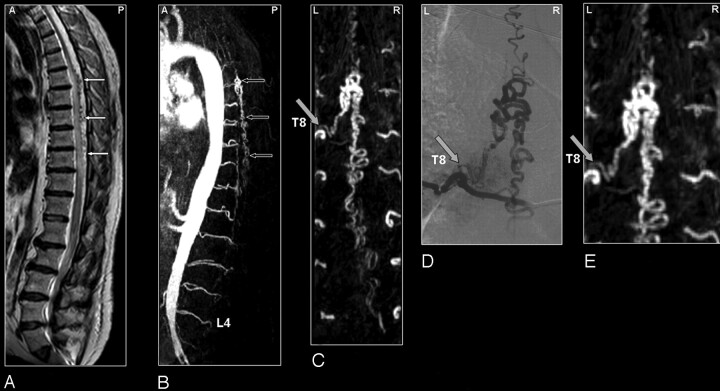
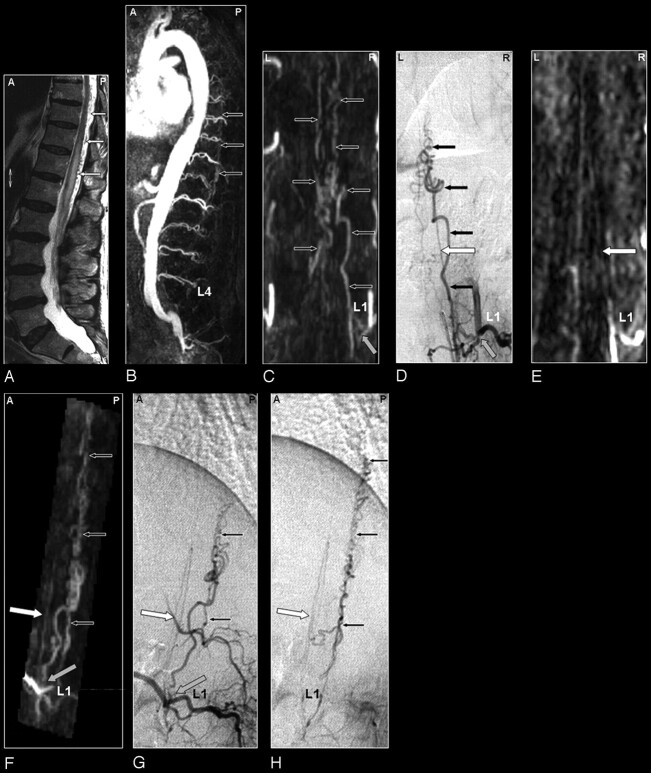
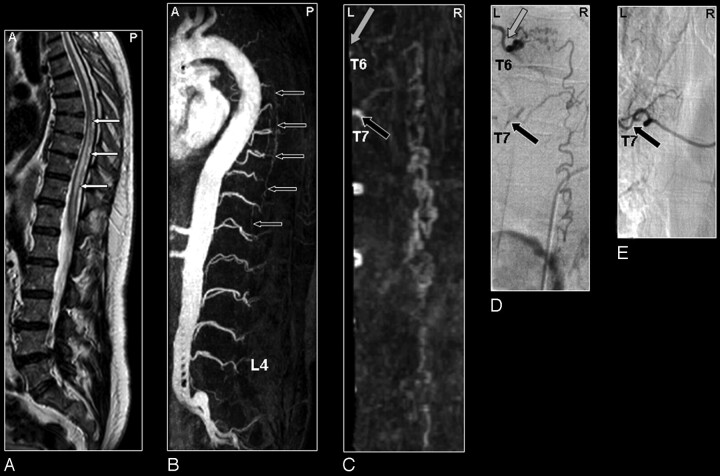
Materials and methods: Thirty-four consecutive patients with suspicion of spinal vascular abnormalities underwent digital subtraction angiography (DSA) after MRA. The level and side of the suspected spinal dural arteriovenous fistula (SDAVF) and the feeding arteries in spinal arteriovenous malformations (SAVMs) were determined from the MRA and compared with DSA.
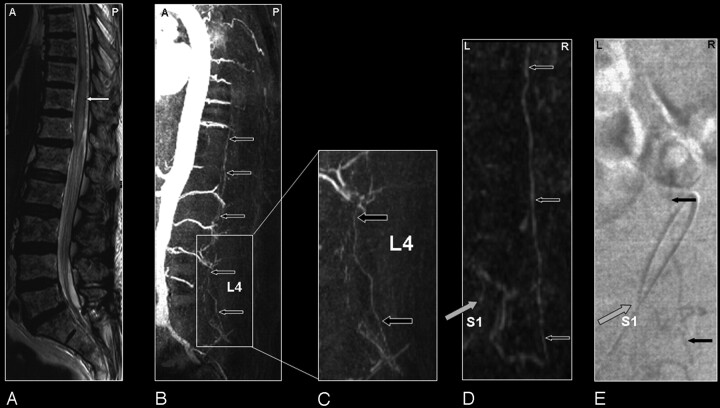
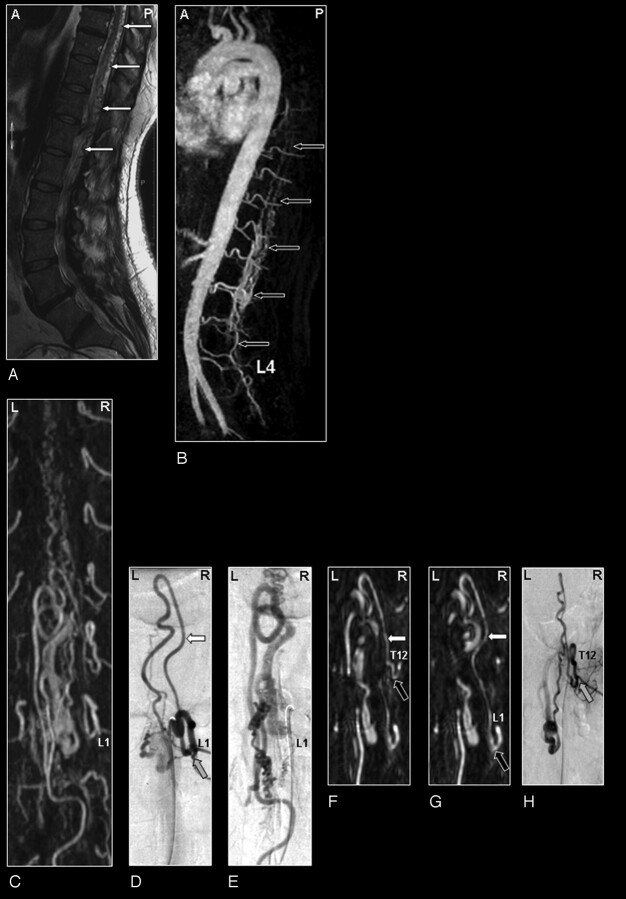
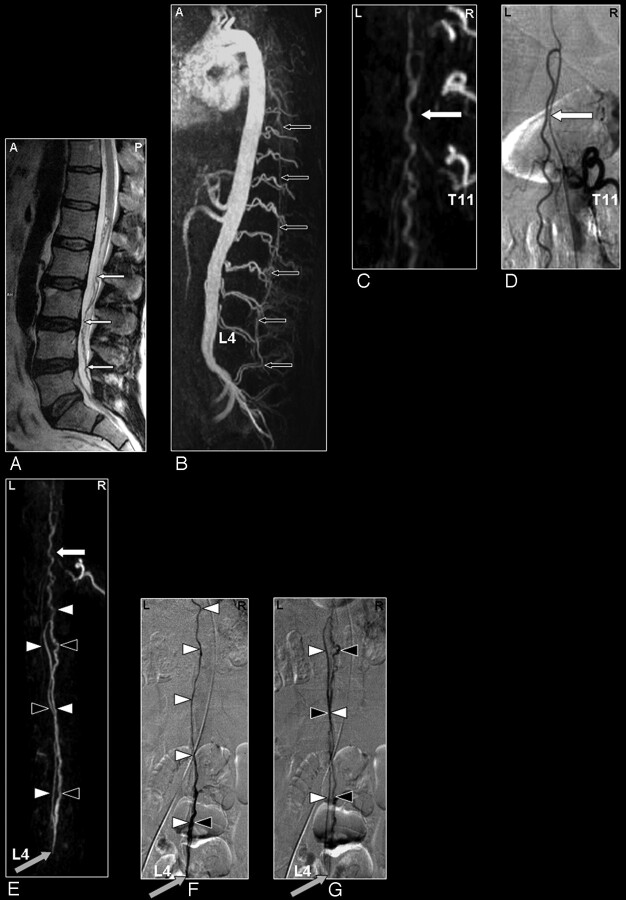
Results: DSA revealed SDAVF in 20 abnormalities of which 19 were spinal and 1 was tentorial with spinal drainage, as well as SAVM in 11 patients. In 3 patients, MRA and DSA were both normal. For detection of spinal arteriovenous abnormalities, neither false-positive nor false-negative MRA results were obtained. The MRA-derived level of the feeding artery in SDAVF agreed with DSA in 14 of 19 cases. In 5 cases, a mismatch of 1 vertebral level (not side) was noted for the feeding artery. For the tentorial AVF, only the spinal drainage was depicted; the feeding artery was outside the MRA field of view. In intradural SAVM, the main feeding artery was identified by MRA in 10 of 11 patients. MRA could differentiate between glomerular and fistulous SAVM in 4 of 6 cases and between sacral SDAVF and filum terminale SAVM in 2 of 5 cases.
Conclusions: MRA reliably detects or excludes various types of spinal AV abnormalities and localizes the (predominant) arterial feeder of most spinal AV shunts. Although classification of the subtype of SAVMs remains difficult, with MRA it greatly helps to focus subsequent DSA.
Figures
Comment in
-
Investigating vascular myelopathy--when can magnetic resonance angiography replace digital subtraction angiography?Nat Clin Pract Neurol. 2008 May;4(5):244-5. doi: 10.1038/ncpneuro0747. Epub 2008 Feb 19. Nat Clin Pract Neurol. 2008. PMID: 18285750 No abstract available.
Similar articles
-
Dynamic contrast-enhanced magnetic resonance angiography for the localization of spinal dural arteriovenous fistulas at 3T.J Neuroradiol. 2017 Feb;44(1):17-23. doi: 10.1016/j.neurad.2016.10.002. Epub 2016 Nov 1. J Neuroradiol. 2017. PMID: 27814888
-
Value of spinal high temporal/high spatial resolution CE-MRA in the diagnosis of spinal dural arteriovenous fistulas.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024 Dec 28;49(12):1927-1933. doi: 10.11817/j.issn.1672-7347.2024.240391. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 40195665 Free PMC article. Chinese, English.
-
The accuracy and utility of contrast-enhanced MR angiography for localization of spinal dural arteriovenous fistulas: the Toronto experience.Eur Radiol. 2014 Nov;24(11):2885-94. doi: 10.1007/s00330-014-3307-6. Epub 2014 Jul 12. Eur Radiol. 2014. PMID: 25015136
-
MR angiography of the spine and spinal cord.Top Magn Reson Imaging. 2003 Dec;14(6):444-60. doi: 10.1097/00002142-200312000-00003. Top Magn Reson Imaging. 2003. PMID: 14872165 Review.
-
Concomitant Sacral Dural Arteriovenous Fistula and Conus Medullaris Arteriovenous Malformation with Respective Drainage Veins: Case Report and Literature Review.World Neurosurg. 2020 Sep;141:299-305. doi: 10.1016/j.wneu.2020.06.022. Epub 2020 Jun 11. World Neurosurg. 2020. PMID: 32535050 Review.
Cited by
-
Novalis Stereotactic Radiosurgery for Spinal Dural Arteriovenous Fistula.J Korean Neurosurg Soc. 2016 Jul;59(4):420-4. doi: 10.3340/jkns.2016.59.4.420. Epub 2016 Jul 8. J Korean Neurosurg Soc. 2016. PMID: 27446527 Free PMC article.
-
Comparison of Time-Resolved and First-Pass Contrast-Enhanced MR Angiography in Pretherapeutic Evaluation of Spinal Dural Arteriovenous Fistulas.AJNR Am J Neuroradiol. 2017 Jan;38(1):206-212. doi: 10.3174/ajnr.A4962. Epub 2016 Nov 3. AJNR Am J Neuroradiol. 2017. PMID: 27811132 Free PMC article.
-
Long-Term Outcome of Patients with Spinal Dural Arteriovenous Fistula: The Dilemma of Delayed Diagnosis.AJNR Am J Neuroradiol. 2020 Feb;41(2):357-363. doi: 10.3174/ajnr.A6372. Epub 2020 Jan 9. AJNR Am J Neuroradiol. 2020. PMID: 31919141 Free PMC article.
-
Clinical utility of optimized three-dimensional T1-, T2-, and T2*-weighted sequences in spinal magnetic resonance imaging.Jpn J Radiol. 2017 Apr;35(4):135-144. doi: 10.1007/s11604-017-0621-3. Epub 2017 Feb 23. Jpn J Radiol. 2017. PMID: 28233194 Review.
-
Advanced noninvasive imaging of spinal vascular malformations.Neurosurg Focus. 2009 Jan;26(1):E9. doi: 10.3171/FOC.2009.26.1.E9. Neurosurg Focus. 2009. PMID: 19119895 Free PMC article. Review.
References
-
- Berenstein A, Lasjaunias P. Spine and spinal cord vascular lesions. In: Surgical Neuroangiography. Vol 5. Berlin: Springer-Verlag;1992. :1–85
-
- Thron AK. Vascular anatomy of the spinal cord. Wien, New York: Springer-Verlag;1988. :3–5
-
- Brandt T, Caplan LR, Dichgans J, et al. Vascular malformations and interventional neuradiology of the spinal cord. In: Brandt T, et al, eds. Neurological Disorders Course and Treatment. 2nd ed. Boston: Academic Press;2003. :517–28
-
- Forbes G, Nichols DA, Jack CR Jr, et al. Complications of spinal cord arteriography: prospective assessment of risk for diagnostic procedures. Radiology 1988;169:479–84 - PubMed
-
- Krings T, Mull M, Gilsbach JM, et al. Spinal vascular malformations. Eur Radiol 2005;15:267–78 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical