

Measuring elevated microvascular permeability and predicting hemorrhagic transformation in acute ischemic stroke using first-pass dynamic perfusion CT imaging
- PMID: 17698530
- PMCID: PMC7977671
- DOI: 10.3174/ajnr.A0539
Measuring elevated microvascular permeability and predicting hemorrhagic transformation in acute ischemic stroke using first-pass dynamic perfusion CT imaging
Abstract
Background and purpose: Hemorrhagic transformation (HT) can be a devastating complication of acute ischemic stroke (AIS). The purpose of this study was to determine whether increased microvascular permeability (PS) of the blood-brain barrier was detected in early AIS by using first-pass dynamic perfusion CT (PCT) and whether PS was significantly higher in infarcts destined for HT.
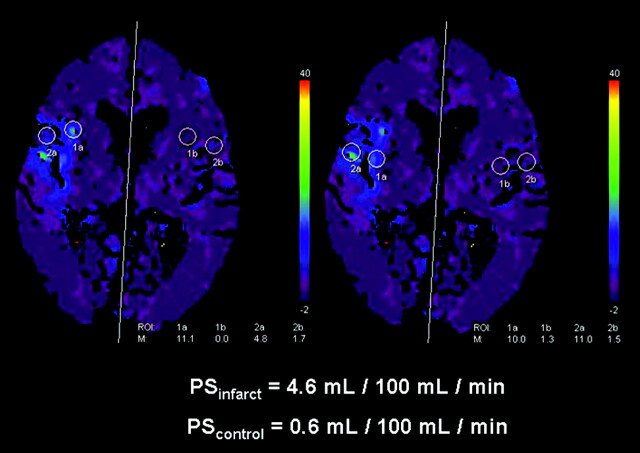
Materials and methods: Fifty patients with AIS less than 3 hours old and evaluated by PCT were included. PS color maps were retrospectively generated from PCT data using the Patlak model. One reader analyzed each PS map by drawing 4 circular 10-mm regions of interest on any focal abnormality. The mean of these 4 regions of interest represented the PS of the infarct (PSinfarct). The mean of 4 mirror regions of interest on the nonischemic contralateral hemisphere was also obtained (PScontrol). PSinfarct and PScontrol were compared by using an exact Wilcoxon test. PSinfarct for infarcts that developed HT on follow-up (PSHT) was compared with all of the others (PSNo-HT) using an exact Mann-Whitney test.
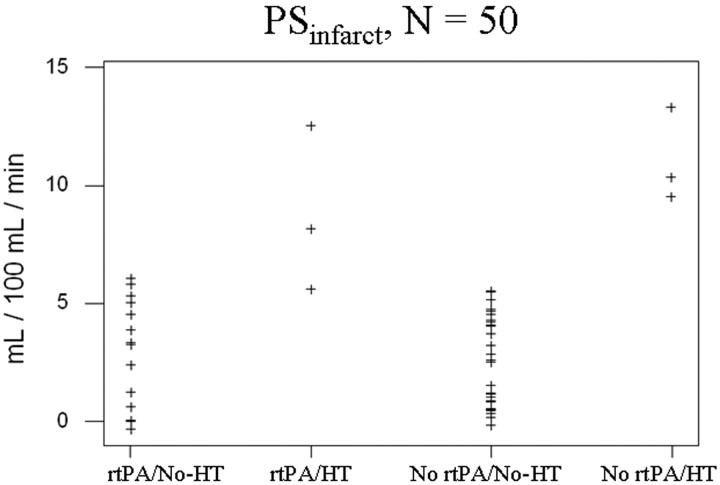
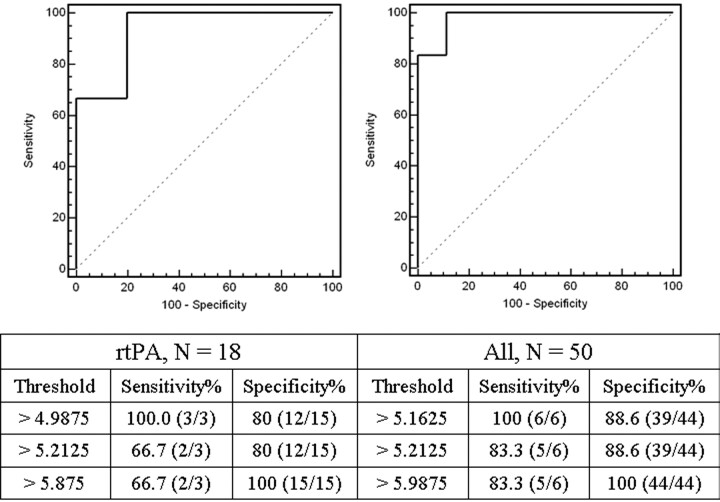
Results: Forty-four infarcts (88%) showed focal PS elevation in the region of infarct. In units of milliliters per 100 milliliters per minute, PSinfarct ranged from 0 to 13 (mean: 3.5+/-3.1) versus PScontrol of 0-0.8 (mean: 0.28+/-0.27; P<.0001). Six infarcts (12%) developed HT, all of which were within the region of PS elevation. PSHT ranged from 5.2 to 13 (mean: 9.8+/-2.9) versus PSNo-HT of 0-5.9 (mean: 2.7+/-2.0; P<.0001). Eighteen infarcts (36%) were treated with recombinant tissue plasminogen activator (rtPA). A significant difference between PSHT and PSNo-HT persisted irrespective of rtPA treatment.
Conclusions: Elevated permeability was detectable in AIS by using first-pass PCT and it predicted subsequent HT.
Figures
References
-
- Axel L. Cerebral blood flow determination by rapid-sequence computed tomography. Radiology 1980;137:679–86 - PubMed
-
- Koenig M, Klotz E, Luka B, et al. Perfusion CT of the brain: diagnostic approach for early detection of ischemic stroke. Radiology 1998;209:85–93 - PubMed
-
- Klotz E, König M. Perfusion measurements of the brain: using dynamic CT for the quantitative assessment of cerebral ischemia in acute stroke. Eur J Radiol 1999;30:170–84 - PubMed
-
- Rother J, Jonetz-Mentzel L, Fiala A, et al. Hemodynamic assessment of acute stroke using dynamic single-slice computed tomographic perfusion imaging. Arch Neurol 2000;57:1161–66 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical