

Distinct imaging patterns and lesion distribution in posterior reversible encephalopathy syndrome
- PMID: 17698535
- PMCID: PMC7977645
- DOI: 10.3174/ajnr.A0549
Distinct imaging patterns and lesion distribution in posterior reversible encephalopathy syndrome
Abstract
Background and purpose: Although the term posterior reversible encephalopathy syndrome (PRES) was popularized because of the typical presence of vasogenic edema in the parietal and occipital lobes, other regions of the brain are also frequently affected. We evaluated lesion distribution with CT and MR in a large cohort of patients who experienced PRES to comprehensively assess the imaging patterns identified.
Materials and methods: The locations of the PRES lesion at toxicity were comprehensively identified and tabulated in 136 patients by CT (22 patients) and MR (114 patients) imaging including the hemispheric, basal ganglial, and infratentorial locations. Clinical associations along with presentation at toxicity including blood pressure were assessed.
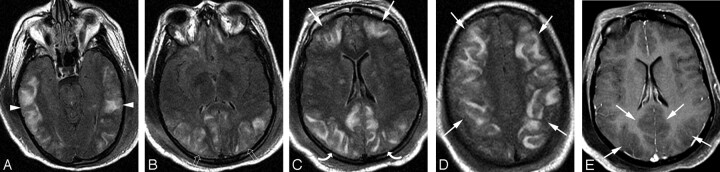
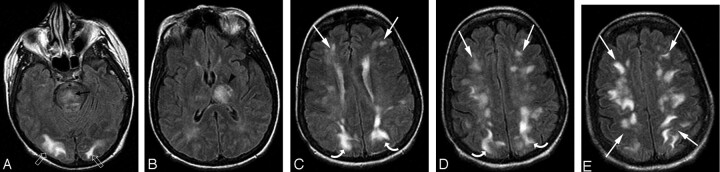
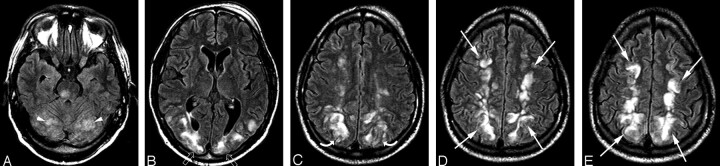
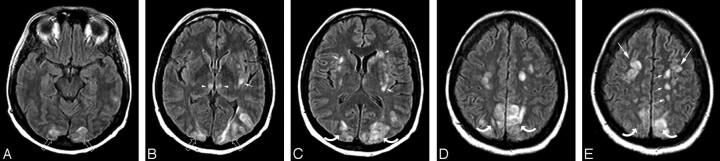
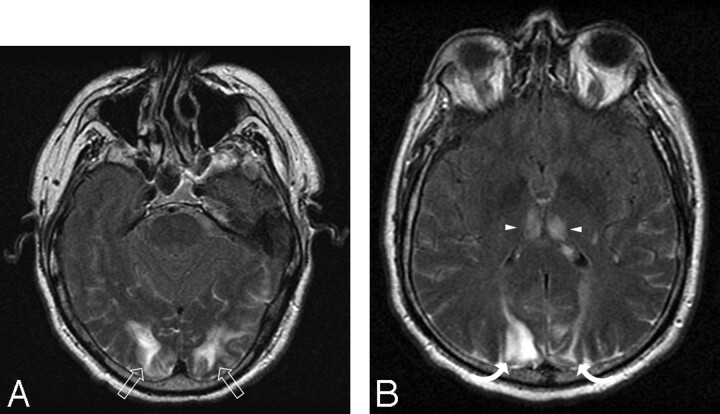
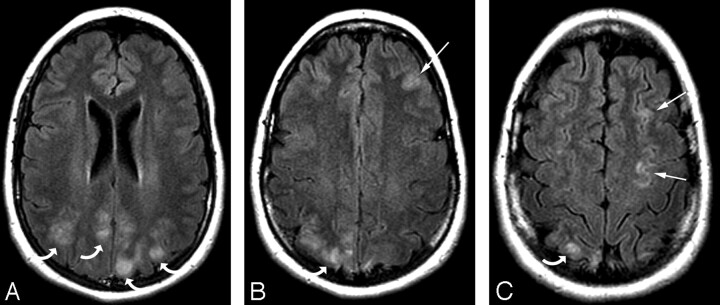
Results: Vasogenic edema was consistently present in the parietal or occipital regions (98%), but other locations were common including the frontal lobes (68%), inferior temporal lobes (40%), and cerebellar hemispheres (30%). Involvement of the basal ganglia (14%), brain stem (13%), and deep white matter (18%) including the splenium (10%) was not rare. Three major patterns of PRES were noted: the holohemispheric watershed (23%), superior frontal sulcal (27%), and dominant parietal-occipital (22%), with additional common partial or asymmetric expression of these primary PRES patterns (28%).
Conclusion: Involvement of the frontal lobe, temporal lobe, and cerebellar hemispheres is common in PRES, along with the occasional presence of lesions in the brain stem, basal ganglia, deep white matter, and splenium. Three primary PRES patterns are noted in the cerebral hemispheres, along with frequent partial or asymmetric expression of these PRES patterns. Awareness of these patterns and variations is important to recognize PRES neurotoxicity more accurately when present.
Figures
References
-
- Sanders TG, Clayman DA, Sanchez-Ramos L, et al. Brain in eclampsia: MR imaging with clinical correlation. Radiology 1991;180:475–78 - PubMed
-
- Schwartz RB, Bravo SM, Klufas RA, et al. Cyclosporine neurotoxicity and its relationship to hypertensive encephalopathy: CT and MR findings in 16 cases. AJR Am J Roentgenol 1995;165:627–31 - PubMed
-
- Bartynski WS, Grabb BC, Zeigler Z, et al. Watershed imaging features and clinical vascular injury in cyclosporin A neurotoxicity. J Comput Assist Tomogr 1997;21:872–80 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources