

Wernicke encephalopathy: MR findings at clinical presentation in twenty-six alcoholic and nonalcoholic patients
- PMID: 17698536
- PMCID: PMC7977668
- DOI: 10.3174/ajnr.A0544
Wernicke encephalopathy: MR findings at clinical presentation in twenty-six alcoholic and nonalcoholic patients
Abstract
Background and purpose: Wernicke encephalopathy is a severe neurologic disorder that results from a dietary vitamin B1 deficiency. It is characterized by changes in consciousness, ocular abnormalities, and ataxia. This study was undertaken to analyze and compare findings on MR imaging and neurologic symptoms at clinical presentations of patients with Wernicke encephalopathy with and without a history of alcohol abuse.
Materials and methods: A multicenter study group retrospectively reviewed MR brain imaging findings, clinical histories, and presentations of 26 patients (14 female, 12 male) diagnosed between 1999 and 2006 with Wernicke encephalopathy. The age range was 6-81 years (mean age, 46 .6+/-19 years).
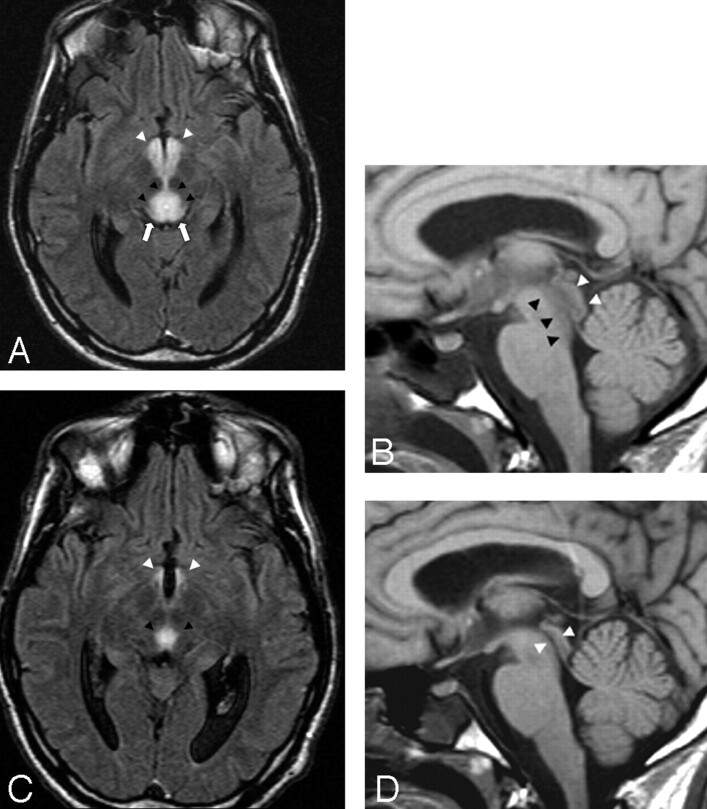
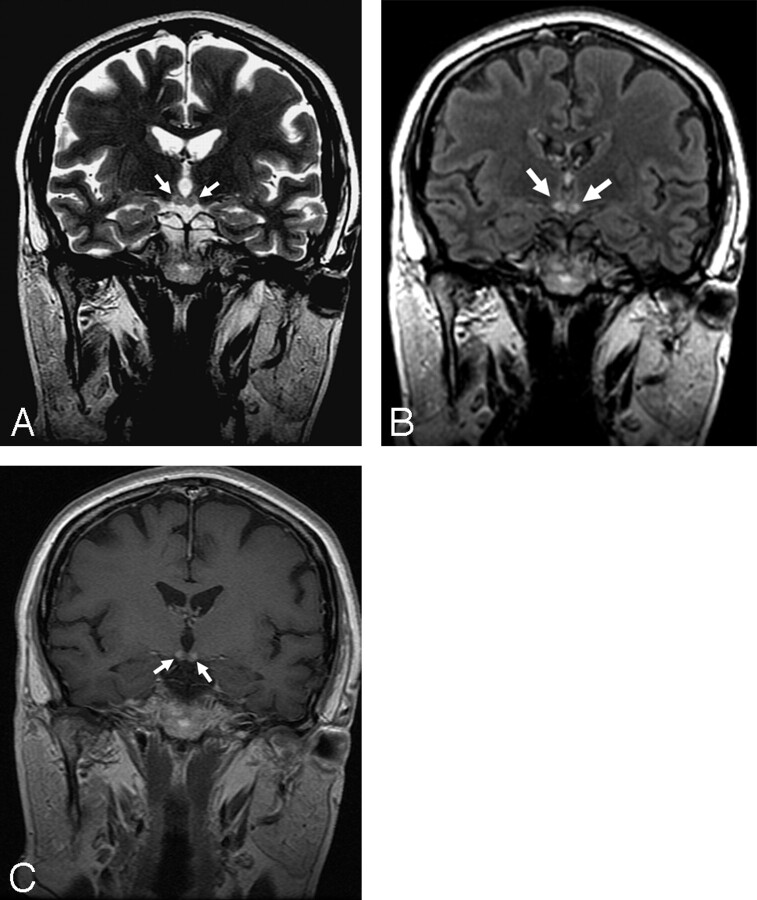
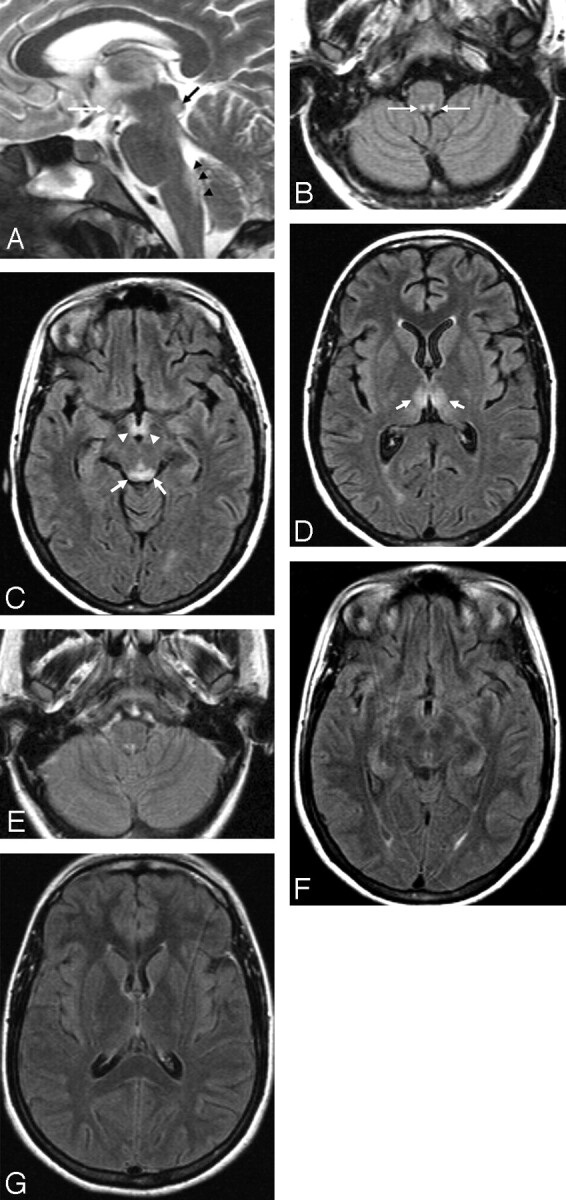
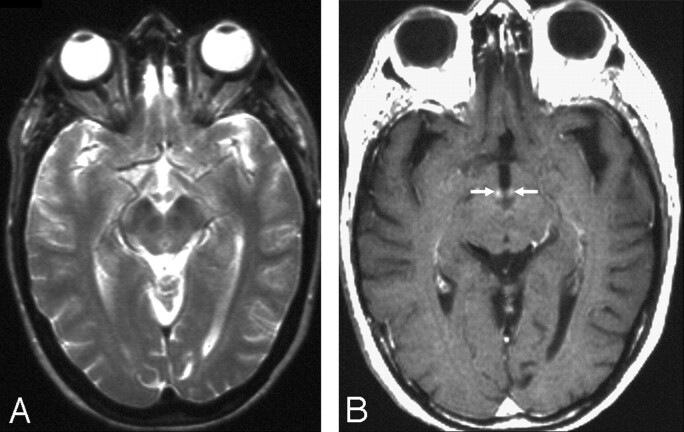
Results: Fifty percent of the patients had a history of alcohol abuse, and 50% had no history of alcohol abuse. Eighty percent showed changes in consciousness, 77% had ocular symptoms, and 54% had ataxia. Only 38% of the patients showed the classic triad of the disease at clinical presentation. At MR examination, 85% of the patients showed symmetric lesions in the medial thalami and the periventricular region of the third ventricle, 65% in the periaqueductal area, 58% in the mamillary bodies, 38% in the tectal plate, and 8% in the dorsal medulla. Contrast enhancement of the mamillary bodies was statistically positively correlated with the alcohol abuse group.
Conclusions: Our study confirms the usefulness of MR in reaching a prompt diagnosis of Wernicke encephalopathy to avoid irreversible damage to brain tissue. Contrast enhancement in the mamillary bodies is a typical finding of the disease in the alcoholic population.
Figures
References
-
- Ogershok PR, Rahman A, Nestor S, et al. Wernicke encephalopathy in nonalcoholic patients. Am J Med Sci 2002;323:107–11 - PubMed
-
- Victor M. The Wernicke-Korsakoff syndrome. In: Vinken PJ, Bruyn GW, eds. Handbook of Clinical Neurology. Vol 28 . Amsterdam: North Holland;1976. :243–70
-
- Harper C, Butterworth R. Nutritional and metabolic disorders. In: Graham DI, Lantos PL, eds. Greenfield's Neuropathology,vol 1 , 6th ed. London: Hodder Arnold;1997. :601–52
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical