

Bone-subtraction CT angiography: evaluation of two different fully automated image-registration procedures for interscan motion compensation
- PMID: 17698541
- PMCID: PMC7977676
- DOI: 10.3174/ajnr.A0558
Bone-subtraction CT angiography: evaluation of two different fully automated image-registration procedures for interscan motion compensation
Abstract
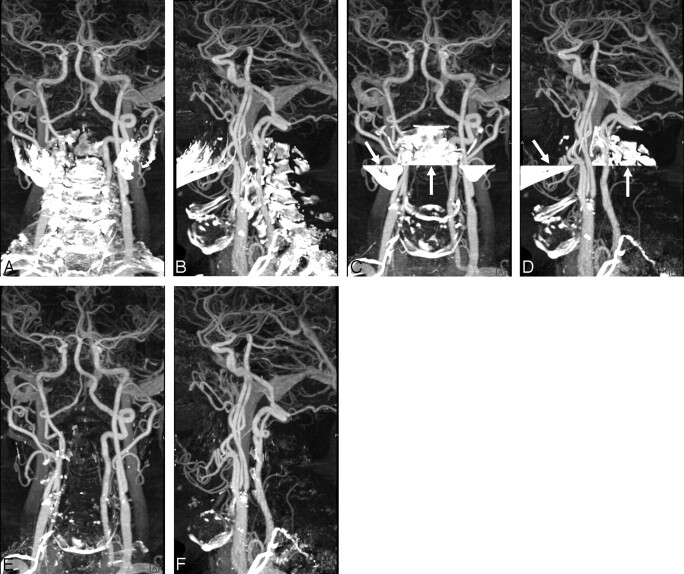
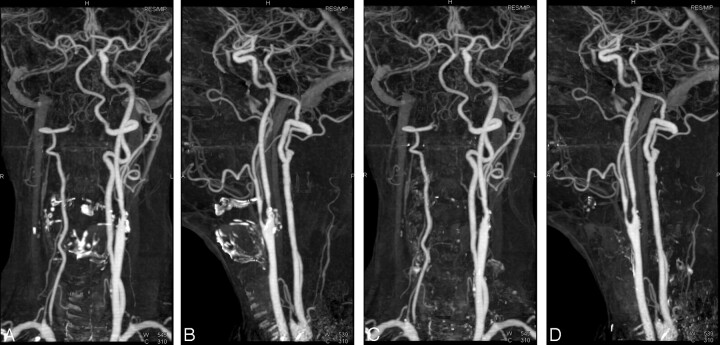
Background and purpose: Bone-subtraction techniques have been shown to enhance CT angiography (CTA) interpretation, but motion can lead to incomplete bone removal. The aim of this study was to evaluate 2 novel registration techniques to compensate for patient motion.
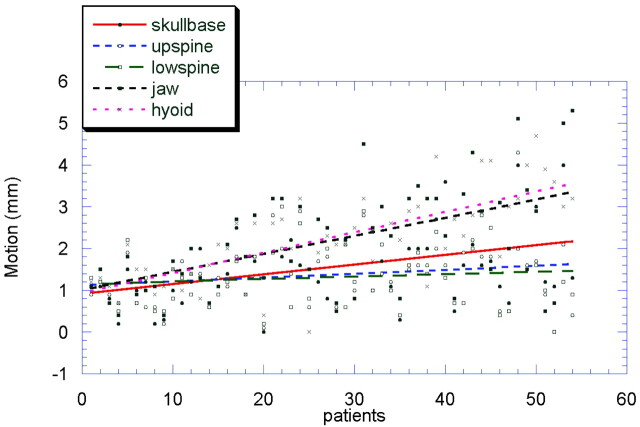
Materials and methods: Fifty-four patients underwent bone-subtraction CTA (BSCTA) for the evaluation of the neck vessels with 64-section CT. We tested 3 different registration procedures: pure rigid registration (BSCTA), slab-based registration (SB-BSCTA), and a partially rigid registration (PR-BSCTA) approach. Subtraction quality for the assessment of different vascular segments was evaluated by 2 examiners in a blinded fashion. The Cohen kappa test was applied for interobserver variability, and the Wilcoxon signed rank test, for differences between the procedures. Motion between the corresponding datasets was measured and plotted against image-quality scores.
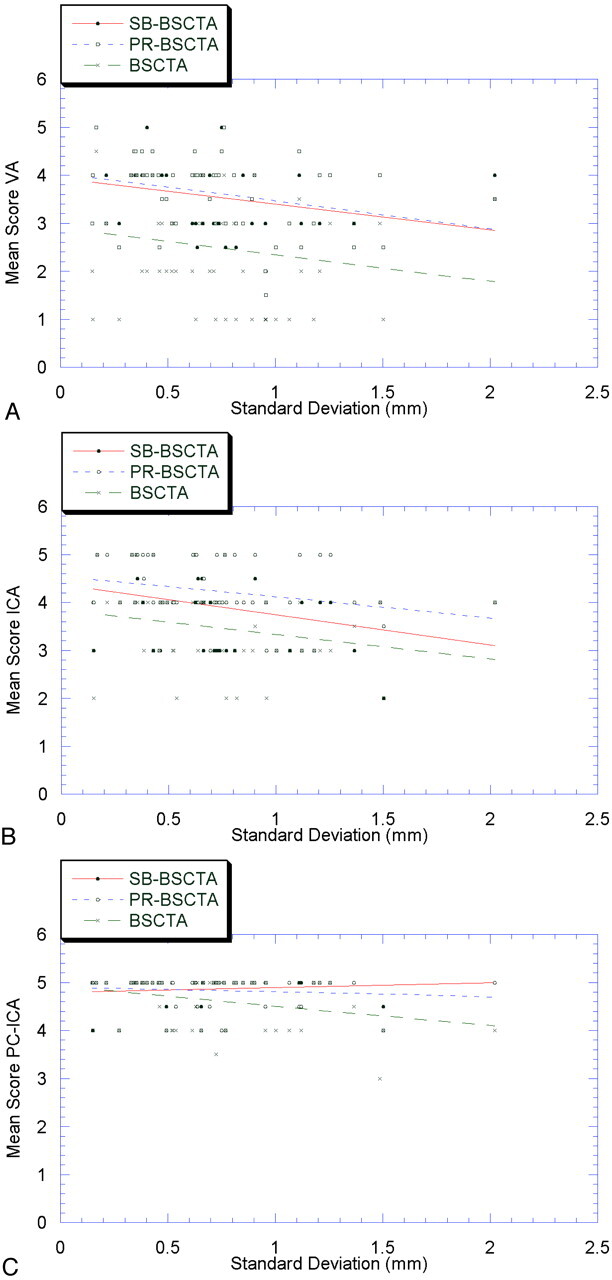
Results: Algorithms with motion compensation revealed higher image-quality scores (SB-BSCTA, mean 4.31; PR-BSCTA, mean 4.43) than pure rigid registration (BSCTA, mean 3.88). PR-BSCTA was rated superior to SB-BSCTA for the evaluation of the cervical internal and external carotid arteries (P<.001), whereas there was no significant difference for the other vessels (P=.157-.655). Both algorithms were clearly superior to pure rigid registration for all vessels except the basilar and ophthalmic artery. Interobserver agreement was high (kappa=0.46-0.98).
Conclusion: Bone-subtraction algorithms with motion compensation provided higher image-quality scores than pure rigid registration methods, especially in cases with complex motion. PR-BSCTA was rated superior to SB-BSCTA in the visualization of the internal and external carotid arteries.
Figures

References
-
- Achenbach S, Ropers D, Pohle FK, et al. Detection of coronary artery stenoses using multi-detector CT with 16 × 0.75 collimation and 375 ms rotation. Eur Heart J 2005;26:1978–86. Epub 2005 May 27 - PubMed
-
- Coxson HO, Baile EM, King GG, et al. Diagnosis of subsegmental pulmonary emboli: a multi-center study using a porcine model. J Thorac Imaging 2005;20:24–31 - PubMed
-
- Ghersin E, Litmanovich D, Dragu R, et al. 16-MDCT coronary angiography versus invasive coronary angiography in acute chest pain syndrome: a blinded prospective study. AJR Am J Roentgenol 2006;186:177–84 - PubMed
-
- Kanne JP, Lalani TA. Role of computed tomography and magnetic resonance imaging for deep venous thrombosis and pulmonary embolism. Circulation 2004;10(12 suppl 1):I15–21 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials