

Circulating and cellular adiponectin in polycystic ovary syndrome: relationship to glucose tolerance and insulin action
- PMID: 17706206
- PMCID: PMC7027432
- DOI: 10.1016/j.fertnstert.2007.04.046
Circulating and cellular adiponectin in polycystic ovary syndrome: relationship to glucose tolerance and insulin action
Abstract
Objective: To evaluate serum adiponectin levels and organization into multimers in women with polycystic ovary syndrome (PCOS) and assess relationships between adiponectin, glucose tolerance, and insulin resistance.
Design: In vivo and in vitro study.
Setting: Outpatient clinic at university and Veterans hospitals in the United States and university laboratory.
Patient(s): Thirty-one obese women with PCOS and six age- and body mass index (BMI)-matched normal cycling control subjects.
Intervention(s): All subjects studied in the fasting state.
Main outcome measure(s): A 75-g oral glucose tolerance test (OGTT), hyperinsulinemic/euglycemic clamp, circulating adiponectin levels, adipocyte adiponectin content, and organization of adiponectin into multimeric forms.
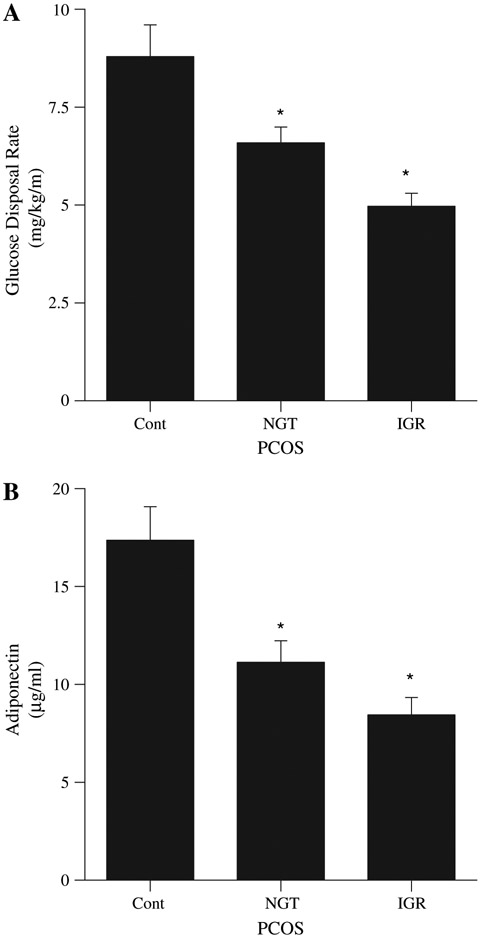
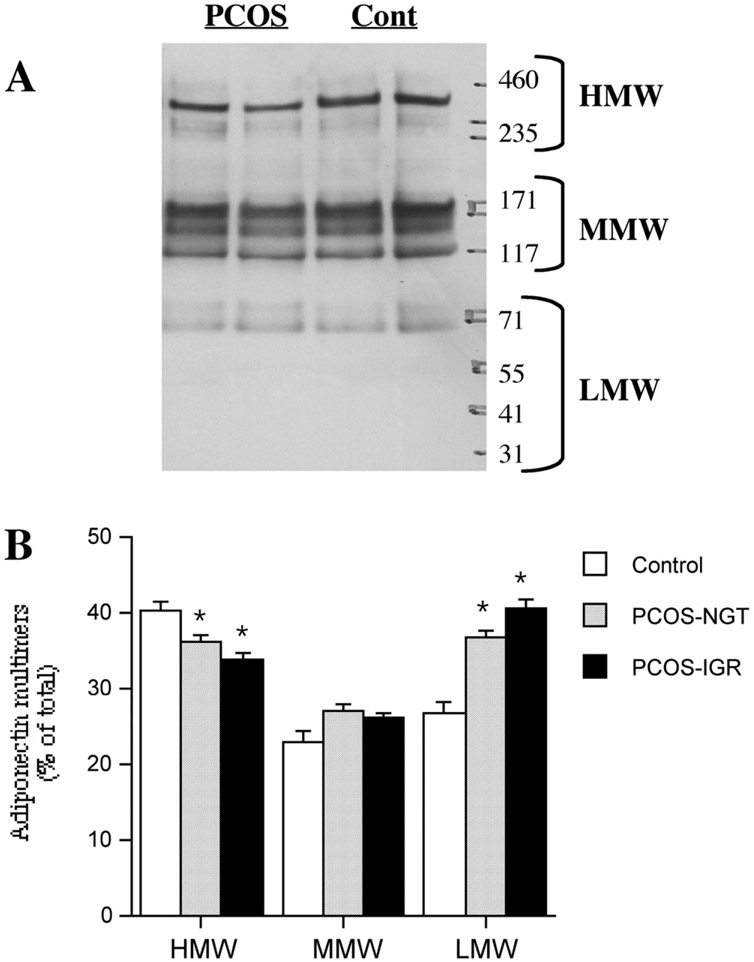
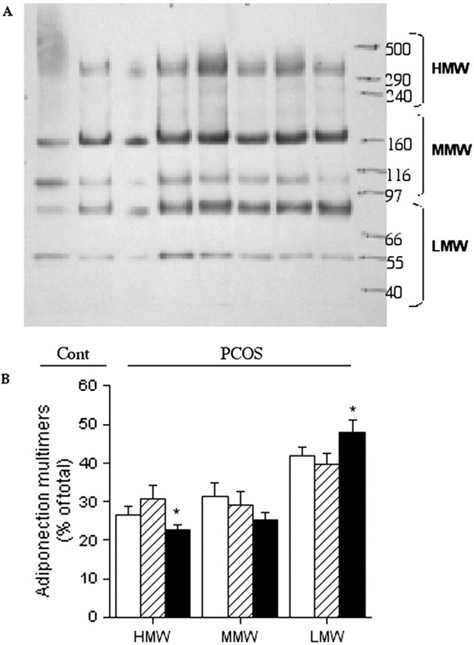
Result(s): Whole body insulin action (glucose disposal rate, 5.61 +/- 2.90 vs. 8.79 +/- 0.81 mg/kg/min, PCOS and control) and adiponectin levels (9.5 +/- 0.7 7 vs. 17.4 +/- 1 microg/mL, PCOS vs. control) were significantly reduced in the subjects with PCOS. There were significant correlations between glucose tolerance, insulin action, and circulating adiponectin levels in all subjects. The content of adiponectin protein was reduced in subcutaneous adipocytes from subjects with PCOS (252 +/- 31 vs. 388 +/- 58 arbitrary units/10 microg protein). Subjects with PCOS had less of their circulating adiponectin organized into high molecular weight (HMW) multimeric complexes. Glucose-intolerant subjects with PCOS also had less intracellular HMW adiponectin.
Conclusion(s): Both circulating adiponectin levels and the portion present as the most active HMW form are reduced in PCOS, with differences related to the degree of glucose intolerance and insulin resistance.
Figures
Comment in
-
Oligo-ovulation or anovulation and hyperandrogenemia contribute to the decreased serum adiponectin levels in normal-weight women with PCOS with obesity and insulin resistance.Fertil Steril. 2009 Apr;91(4):e3; author reply e4. doi: 10.1016/j.fertnstert.2008.12.075. Epub 2009 Feb 24. Fertil Steril. 2009. PMID: 19243758 No abstract available.
References
-
- Knochenhauer ES, Key TJ, Kahsar-Miller M, Waggoner W, Boots LR, Azziz R. Prevalence of the polycystic ovary syndrome in unselected black and white women of the southeastern United States: a prospective study. J Clin Endo Metabol 1998;83:3078–82. - PubMed
-
- Chang RJ, Nakamura RM, Judd HL, Kaplan SA. Insulin resistance in nonobese patients with polycystic ovarian disease. J Clin Endocrinol Metab 1983;57:356–9. - PubMed
-
- Cattrall FR, Healy DL. Long-term metabolic, cardiovascular and neoplastic risks with polycystic ovarian syndrome. Best Pract Res Clin Obstet Gynaecol 2004;18:803–12. - PubMed
-
- Kershaw EE, Flier JS. Adipose tissue as an endocrine organ. J Clin Endocrinol Metab 2004;89:2548–56. - PubMed
-
- Daimon M, Oizumi T, Saitoh T, Kameda W, Hirata A, Yamaguchi H, et al. Decreased serum levels of adiponectin are a risk factor for the progression to type 2 diabetes in the Japanese population: the Funagata study. Diabetes Care 2003;26:2015–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
