

Relapse following discontinuation of imatinib mesylate therapy for FIP1L1/PDGFRA-positive chronic eosinophilic leukemia: implications for optimal dosing
- PMID: 17709602
- PMCID: PMC2077306
- DOI: 10.1182/blood-2007-07-100164
Relapse following discontinuation of imatinib mesylate therapy for FIP1L1/PDGFRA-positive chronic eosinophilic leukemia: implications for optimal dosing
Abstract
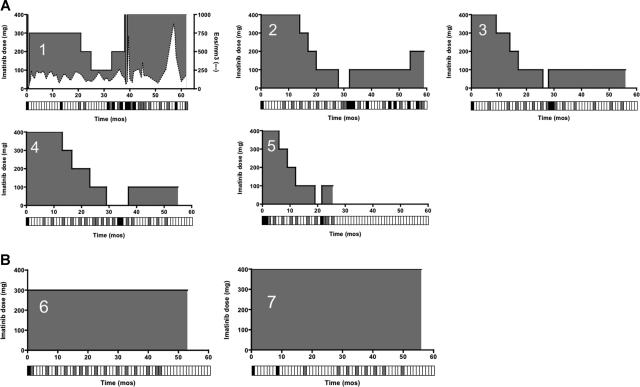
Although imatinib is clearly the treatment of choice for FIP1L1/PDGFRA-positive chronic eosinophilic leukemia (CEL), little is known about optimal dosing, duration of treatment, and the possibility of cure in this disorder. To address these questions, 5 patients with FIP1L1/PDGFRA-positive CEL with documented clinical, hematologic, and molecular remission on imatinib (400 mg daily) and without evidence of cardiac involvement were enrolled in a dose de-escalation trial. The imatinib dose was tapered slowly with close follow-up for evidence of clinical, hematologic, and molecular relapse. Two patients with endomyocardial fibrosis were maintained on imatinib 300 to 400 mg daily and served as controls. All 5 patients who underwent dose de-escalation, but neither of the control patients, experienced molecular relapse (P < .05). None developed recurrent symptoms, and eosinophil counts, serum B12, and tryptase levels remained suppressed. Reinitiation of therapy at the prior effective dose led to molecular remission in all 5 patients, although 2 patients subsequently required increased dosing to maintain remission. These data are consistent with suppression rather than elimination of the clonal population in FIP1L1/PDGFRA-positive CEL and suggest that molecular monitoring may be the most useful method in determining optimal dosing without the risk of disease exacerbation. This trial was registered at http://www.clinicaltrials.gov as no. NCT00044304.
Figures
Similar articles
-
Isolated molecular relapse in FIP1L1-PDGFRalpha hypereosinophilic syndrome after discontinuation and single weekly dose of imatinib: need of quantitative molecular procedures to modulate imatinib dose.Cancer Chemother Pharmacol. 2009 May;63(6):1161-3. doi: 10.1007/s00280-008-0858-8. Epub 2008 Nov 7. Cancer Chemother Pharmacol. 2009. PMID: 18989670
-
Successful imatinib treatment of cardiac involvement of FIP1L1-PDGFRA-positive chronic eosinophilic leukemia followed by severe hepatotoxicity.Int J Hematol. 2007 Oct;86(3):233-7. doi: 10.1532/IJH97.07032. Int J Hematol. 2007. PMID: 17988989 Review.
-
Maintenance therapy with imatinib appears necessary despite molecular remission in FIP1L1-PDGFRA fusion gene positive hypereosinophilic disorder.Leuk Res. 2008 Jan;32(1):169-71. doi: 10.1016/j.leukres.2007.04.004. Epub 2007 Jun 4. Leuk Res. 2008. PMID: 17544504
-
A single weekly dose of imatinib is sufficient to induce and maintain remission of chronic eosinophilic leukaemia in FIP1L1-PDGFRA-expressing patients.Br J Haematol. 2008 Apr;141(2):200-4. doi: 10.1111/j.1365-2141.2008.07033.x. Epub 2008 Feb 26. Br J Haematol. 2008. PMID: 18307562 Clinical Trial.
-
FIP1L1-PDGFR alpha, a therapeutic target for the treatment of chronic eosinophilic leukemia.Verh K Acad Geneeskd Belg. 2005;67(3):169-76. Verh K Acad Geneeskd Belg. 2005. PMID: 16089297 Review.
Cited by
-
Clinical overview of cutaneous features in hypereosinophilic syndrome.Curr Allergy Asthma Rep. 2012 Apr;12(2):85-98. doi: 10.1007/s11882-012-0241-z. Curr Allergy Asthma Rep. 2012. PMID: 22359067 Review.
-
How I treat hypereosinophilic syndromes.Blood. 2015 Aug 27;126(9):1069-77. doi: 10.1182/blood-2014-11-551614. Epub 2015 May 11. Blood. 2015. PMID: 25964669 Free PMC article. Review.
-
Novel Therapies for Eosinophilic Disorders.Immunol Allergy Clin North Am. 2015 Aug;35(3):577-98. doi: 10.1016/j.iac.2015.05.007. Immunol Allergy Clin North Am. 2015. PMID: 26209901 Free PMC article. Review.
-
Advances in diagnosis and treatment of eosinophilia.Curr Opin Hematol. 2009 Jan;16(1):3-8. doi: 10.1097/MOH.0b013e32831c841f. Curr Opin Hematol. 2009. PMID: 19057198 Free PMC article. Review.
-
Clinical and Biological Markers in Hypereosinophilic Syndromes.Front Med (Lausanne). 2017 Dec 22;4:240. doi: 10.3389/fmed.2017.00240. eCollection 2017. Front Med (Lausanne). 2017. PMID: 29312946 Free PMC article.
References
-
- Hughes TP, Kaeda J, Branford S, et al. Frequency of major molecular responses to imatinib or interferon alpha plus cytarabine in newly diagnosed chronic myeloid leukemia. N Engl J Med. 2003;349:1423–1432. - PubMed
-
- Bhatia R, Holtz MS, Niu N, et al. Persistence of malignant hematopoietic progenitors in chronic myelogenous leukemia patients in complete cytogenetic remission following imatinib mesylate treatment. Blood. 2003;101:4701–4707. - PubMed
-
- Graham SM, Jorgensen HG, Allan E, et al. Primitive, quiescent, Philadelphia-positive stem cells from patients with chronic myeloid leukemia are insensitive to STI571 in vitro. Blood. 2002;99:319–325. - PubMed
-
- Holtz MS, Slovak ML, Zhang F, Sawyers CL, Forman SJ, Bhatia R. Imatinib mesylate (STI571) inhibits growth of primitive malignant progenitors in chronic myelogenous leukemia through reversal of abnormally increased proliferation. Blood. 2002;99:3792–3800. - PubMed
-
- Chu S, Xu H, Shah NP, et al. Detection of BCR-ABL kinase mutations in CD34+ cells from chronic myelogenous leukemia patients in complete cytogenetic remission on imatiinb mesylate therapy. Blood. 2005;105:2093–2098. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
