

Stress and wound healing
- PMID: 17709956
- PMCID: PMC2792763
- DOI: 10.1159/000104862
Stress and wound healing
Abstract
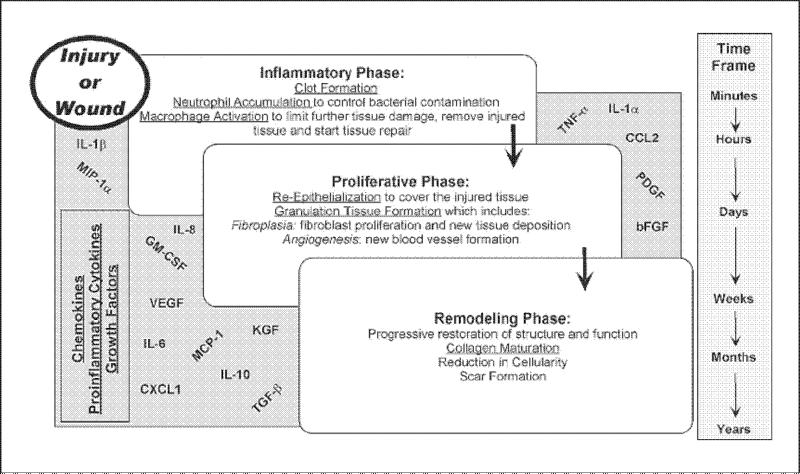
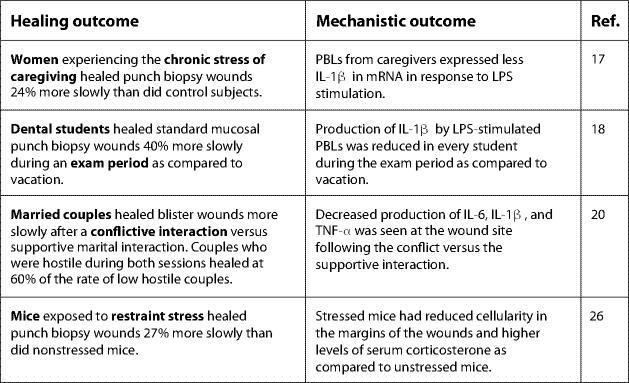
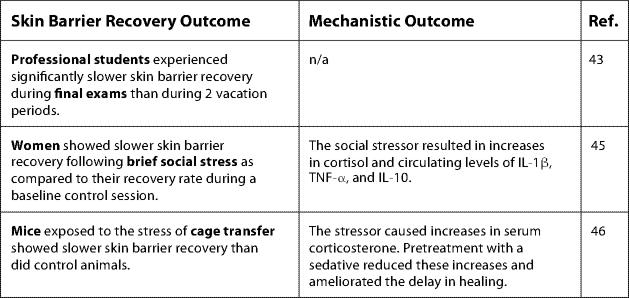
Over the past decade it has become clear that stress can significantly slow wound healing: stressors ranging in magnitude and duration impair healing in humans and animals. For example, in humans, the chronic stress of caregiving as well as the relatively brief stress of academic examinations impedes healing. Similarly, restraint stress slows healing in mice. The interactive effects of glucocorticoids (e.g. cortisol and corticosterone) and proinflammatory cytokines [e.g. interleukin-1beta (IL-1beta), IL-1alpha, IL-6, IL-8, and tumor necrosis factor-alpha] are primary physiological mechanisms underlying the stress and healing connection. The effects of stress on healing have important implications in the context of surgery and naturally occurring wounds, particularly among at-risk and chronically ill populations. In research with clinical populations, greater attention to measurement of health behaviors is needed to better separate behavioral versus direct physiological effects of stress on healing. Recent evidence suggests that interventions designed to reduce stress and its concomitants (e.g., exercise, social support) can prevent stress-induced impairments in healing. Moreover, specific physiological mechanisms are associated with certain types of interventions. In future research, an increased focus on mechanisms will help to more clearly elucidate pathways linking stress and healing processes.
Copyright (c) 2006 S. Karger AG, Basel.
Figures
References
-
- Elias PM. Stratum corneum defensive functions: an integrated view. J Invest Dermatol. 2005;125:183–200. - PubMed
-
- Marks R. The stratum corneum barrier: the final frontier. J Nutr. 2004;134:2071S–2021S. - PubMed
-
- Singer AJ, Clark RA. Cutaneous wound healing. N Engl J Med. 1999;341:738–746. - PubMed
-
- Baum CL, Arpey CJ. Normal cutaneous wound healing: clinical correlation with cellular and molecular events. Dermatol Surg. 2005;31:674–686. - PubMed
-
- King SM, Reed GL. Development of platelet secretary granules. Semin Cell Dev Biol. 2002;13:293–302. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
