

Loss of receptor on tuberculin-reactive T-cells marks active pulmonary tuberculosis
- PMID: 17710135
- PMCID: PMC1936433
- DOI: 10.1371/journal.pone.0000735
Loss of receptor on tuberculin-reactive T-cells marks active pulmonary tuberculosis
Abstract
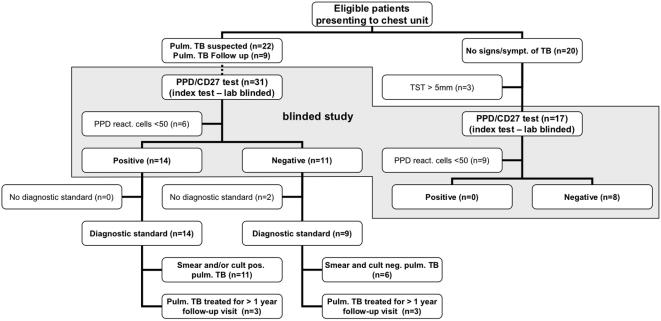
Background: Tuberculin-specific T-cell responses have low diagnostic specificity in BCG vaccinated populations. While subunit-antigen (e.g. ESAT-6, CFP-10) based tests are useful for diagnosing latent tuberculosis infection, there is no reliable immunological test for active pulmonary tuberculosis. Notably, all existing immunological tuberculosis-tests are based on T-cell response size, whereas the diagnostic potential of T-cell response quality has never been explored. This includes surface marker expression and functionality of mycobacterial antigen specific T-cells.
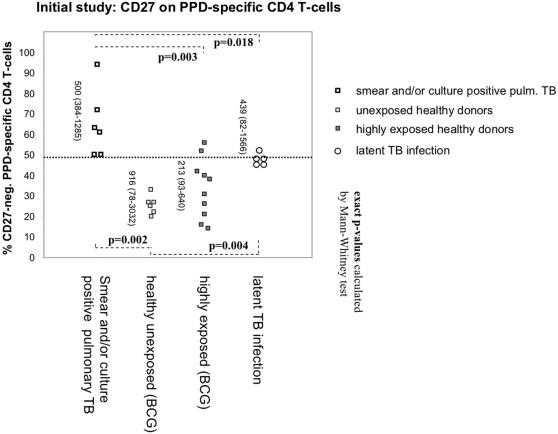
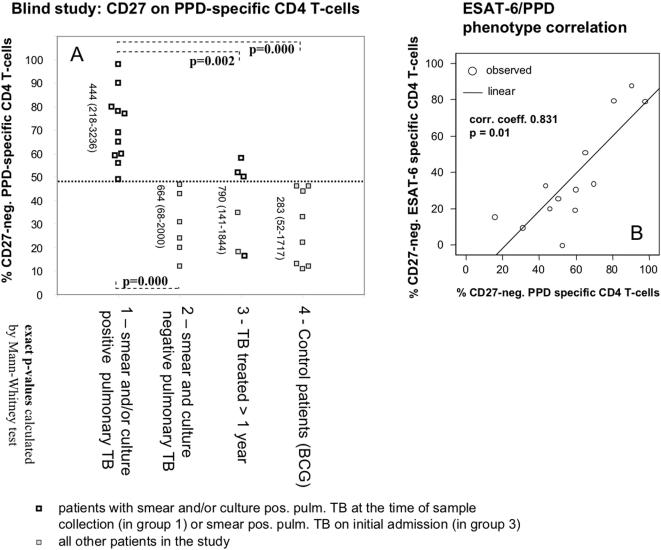
Methodology/principal findings: Flow-cytometry was used to examine over-night antigen-stimulated T-cells from tuberculosis patients and controls. Tuberculin and/or the relatively M. tuberculosis specific ESAT-6 protein were used as stimulants. A set of classic surface markers of T-cell naïve/memory differentiation was selected and IFN-gamma production was used to identify T-cells recognizing these antigens. The percentage of tuberculin-specific T-helper-cells lacking the surface receptor CD27, a state associated with advanced differentiation, varied considerably between individuals (from less than 5% to more than 95%). Healthy BCG vaccinated individuals had significantly fewer CD27-negative tuberculin-reactive CD4 T-cells than patients with smear and/or culture positive pulmonary tuberculosis, discriminating these groups with high sensitivity and specificity, whereas individuals with latent tuberculosis infection exhibited levels in between.
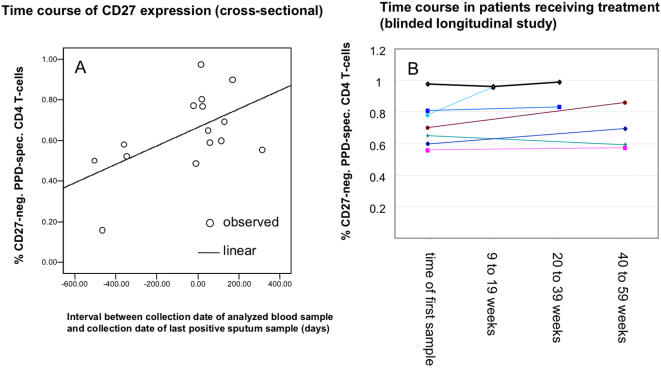
Conclusions/significance: Smear and/or culture positive pulmonary tuberculosis can be diagnosed by a rapid and reliable immunological test based on the distribution of CD27 expression on peripheral blood tuberculin specific T-cells. This test works very well even in a BCG vaccinated population. It is simple and will be of great utility in situations where sputum specimens are difficult to obtain or sputum-smear is negative. It will also help avoid unnecessary hospitalization and patient isolation.
Conflict of interest statement
Figures

Similar articles
-
Tuberculin skin testing compared with T-cell responses to Mycobacterium tuberculosis-specific and nonspecific antigens for detection of latent infection in persons with recent tuberculosis contact.Clin Diagn Lab Immunol. 2001 Nov;8(6):1089-96. doi: 10.1128/CDLI.8.6.1089-1096.2001. Clin Diagn Lab Immunol. 2001. PMID: 11687445 Free PMC article.
-
The phenotypic distribution and functional profile of tuberculin-specific CD4 T-cells characterizes different stages of TB infection.Cytometry B Clin Cytom. 2012 Nov;82(6):360-8. doi: 10.1002/cyto.b.21041. Epub 2012 Sep 7. Cytometry B Clin Cytom. 2012. PMID: 22961735
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
-
Characterization of CD4 and CD8 T cells producing IFN-γ in human latent and active tuberculosis.Tuberculosis (Edinb). 2010 Nov;90(6):346-53. doi: 10.1016/j.tube.2010.09.003. Epub 2010 Oct 8. Tuberculosis (Edinb). 2010. PMID: 20933471
-
The role of flow cytometry in the interferon-gamma-based diagnosis of active tuberculosis and its coinfection with HIV-1--A technically oriented review.Cytometry B Clin Cytom. 2008;74 Suppl 1:S141-51. doi: 10.1002/cyto.b.20381. Cytometry B Clin Cytom. 2008. PMID: 18061950 Review.
Cited by
-
Cell Differentiation Degree as a Factor Determining the Role for Different T-Helper Populations in Tuberculosis Protection.Front Immunol. 2019 May 8;10:972. doi: 10.3389/fimmu.2019.00972. eCollection 2019. Front Immunol. 2019. PMID: 31134070 Free PMC article. Review.
-
Immune response to mycobacterial infection: lessons from flow cytometry.Clin Dev Immunol. 2013;2013:464039. doi: 10.1155/2013/464039. Epub 2013 Nov 27. Clin Dev Immunol. 2013. PMID: 24376464 Free PMC article. Review.
-
Pulmonary immune-compartment-specific interferon gamma responses in HIV-infected individuals with active tuberculosis (TB) in an area of high TB prevalence.Clin Dev Immunol. 2012;2012:308473. doi: 10.1155/2012/308473. Epub 2012 Jun 21. Clin Dev Immunol. 2012. PMID: 22778764 Free PMC article.
-
Rapid diagnosis of smear-negative tuberculosis using immunology and microbiology with induced sputum in HIV-infected and uninfected individuals.PLoS One. 2007 Dec 19;2(12):e1335. doi: 10.1371/journal.pone.0001335. PLoS One. 2007. PMID: 18092001 Free PMC article.
-
Assessment of tuberculosis disease activity in people infected with Mycobacterium tuberculosis and living with HIV: A longitudinal cohort study.EClinicalMedicine. 2022 Jul 13;49:101470. doi: 10.1016/j.eclinm.2022.101470. eCollection 2022 Jul. EClinicalMedicine. 2022. PMID: 35873194 Free PMC article.
References
-
- Lalvani A, Pathan AA, Durkan H, Wilkinson KA, Whelan A, et al. Enhanced contact tracing and spatial tracking of Mycobacterium tuberculosis infection by enumeration of antigen-specific T cells. Lancet. 2001;357:2017–2021. - PubMed
-
- Mazurek GH, Jereb J, Lobue P, Iademarco MF, Metchock B, et al. Guidelines for using the QuantiFERON-TB Gold test for detecting Mycobacterium tuberculosis infection, United States. MMWR Recomm Rep. 2005;54:49–55. - PubMed
-
- Ferrara G, Losi M, D'Amico R, Roversi P, Piro R, et al. Use in routine clinical practice of two commercial blood tests for diagnosis of infection with Mycobacterium tuberculosis: a prospective study. Lancet. 2006;367:1328–1334. - PubMed
-
- Pai M, Riley LW, Colford JM., Jr Interferon-gamma assays in the immunodiagnosis of tuberculosis: a systematic review. Lancet Infect Dis. 2004;4:761–776. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
