

The costs, benefits, and cost-effectiveness of interventions to reduce maternal morbidity and mortality in Mexico
- PMID: 17710149
- PMCID: PMC1939734
- DOI: 10.1371/journal.pone.0000750
The costs, benefits, and cost-effectiveness of interventions to reduce maternal morbidity and mortality in Mexico
Abstract
Background: In Mexico, the lifetime risk of dying from maternal causes is 1 in 370 compared to 1 in 2,500 in the U.S. Although national efforts have been made to improve maternal services in the last decade, it is unclear if Millennium Development Goal 5--to reduce maternal mortality by three-quarters by 2015--will be met.
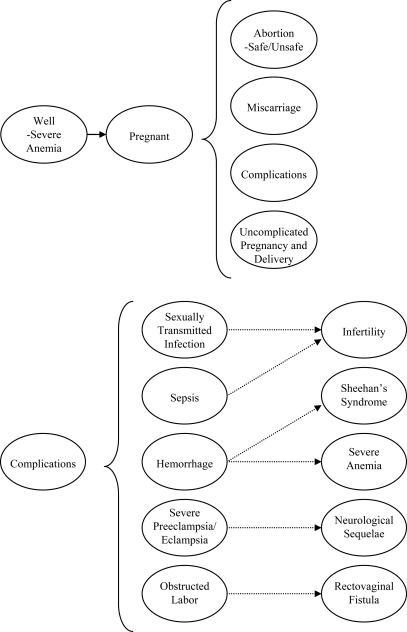
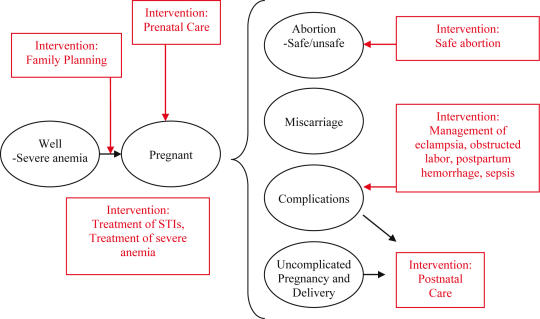
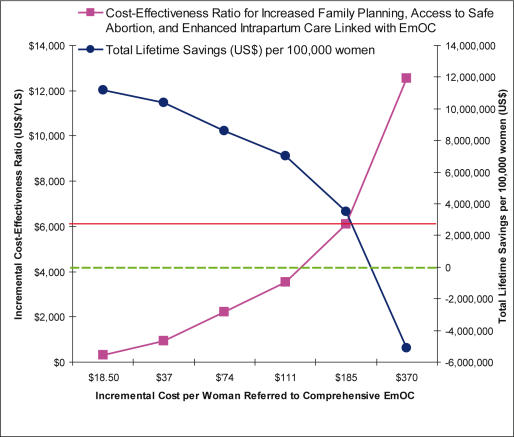
Methodology/principal findings: We developed an empirically calibrated model that simulates the natural history of pregnancy and pregnancy-related complications in a cohort of 15-year-old women followed over their lifetime. After synthesizing national and sub-national trends in maternal mortality, the model was calibrated to current intervention-specific coverage levels and validated by comparing model-projected life expectancy, total fertility rate, crude birth rate and maternal mortality ratio with Mexico-specific data. Using both published and primary data, we assessed the comparative health and economic outcomes of alternative strategies to reduce maternal morbidity and mortality. A dual approach that increased coverage of family planning by 15%, and assured access to safe abortion for all women desiring elective termination of pregnancy, reduced mortality by 43% and was cost saving compared to current practice. The most effective strategy added a third component, enhanced access to comprehensive emergency obstetric care for at least 90% of women requiring referral. At a national level, this strategy reduced mortality by 75%, cost less than current practice, and had an incremental cost-effectiveness ratio of $300 per DALY relative to the next best strategy. Analyses conducted at the state level yielded similar results.
Conclusions/significance: Increasing the provision of family planning and assuring access to safe abortion are feasible, complementary and cost-effective strategies that would provide the greatest benefit within a short-time frame. Incremental improvements in access to high-quality intrapartum and emergency obstetric care will further reduce maternal deaths and disability.
Conflict of interest statement
Figures
Similar articles
-
National and sub-national analysis of the health benefits and cost-effectiveness of strategies to reduce maternal mortality in Afghanistan.Health Policy Plan. 2013 Jan;28(1):62-74. doi: 10.1093/heapol/czs026. Epub 2012 Mar 12. Health Policy Plan. 2013. PMID: 22411880
-
Alternative strategies to reduce maternal mortality in India: a cost-effectiveness analysis.PLoS Med. 2010 Apr 20;7(4):e1000264. doi: 10.1371/journal.pmed.1000264. PLoS Med. 2010. PMID: 20421922 Free PMC article.
-
Triple return on investment: the cost and impact of 13 interventions that could prevent stillbirths and save the lives of mothers and babies in South Africa.BMC Pregnancy Childbirth. 2015 Feb 18;15:39. doi: 10.1186/s12884-015-0456-9. BMC Pregnancy Childbirth. 2015. PMID: 25879579 Free PMC article.
-
The impact of maternal health improvement on perinatal survival: cost-effective alternatives.Int J Health Plann Manage. 1994 Apr-Jun;9(2):131-49. doi: 10.1002/hpm.4740090203. Int J Health Plann Manage. 1994. PMID: 10137136 Review.
-
Maternal health in fifty years of Tanzania independence: Challenges and opportunities of reducing maternal mortality.Tanzan J Health Res. 2011 Dec;13(5 Suppl 1):352-64. doi: 10.4314/thrb.v13i5.5. Tanzan J Health Res. 2011. PMID: 26591990 Review.
Cited by
-
Economic Evaluation of Family Planning Interventions in Low and Middle Income Countries; A Systematic Review.PLoS One. 2016 Dec 19;11(12):e0168447. doi: 10.1371/journal.pone.0168447. eCollection 2016. PLoS One. 2016. PMID: 27992552 Free PMC article.
-
Maternal morbidity: neglected dimension of safe motherhood in the developing world.Glob Public Health. 2012;7(6):603-17. doi: 10.1080/17441692.2012.668919. Epub 2012 Mar 16. Glob Public Health. 2012. PMID: 22424546 Free PMC article.
-
The potential of medical abortion to reduce maternal mortality in Africa: what benefits for Tanzania and Ethiopia?PLoS One. 2010 Oct 11;5(10):e13260. doi: 10.1371/journal.pone.0013260. PLoS One. 2010. PMID: 20948995 Free PMC article.
-
Cost-effectiveness of emergency care interventions in low and middle-income countries: a systematic review.Bull World Health Organ. 2020 May 1;98(5):341-352. doi: 10.2471/BLT.19.241158. Epub 2020 Feb 25. Bull World Health Organ. 2020. PMID: 32514199 Free PMC article.
-
The cost-effectiveness of a program to reduce intrapartum and neonatal mortality in a referral hospital in Ghana.PLoS One. 2020 Nov 13;15(11):e0242170. doi: 10.1371/journal.pone.0242170. eCollection 2020. PLoS One. 2020. PMID: 33186395 Free PMC article.
References
-
- AbouZahr C, Wardlaw T. Maternal mortality in 2000: estimates developed by WHO, UNICEF and UNFPA. Geneva: World Health Organization; 2004. p. 24.
-
- Ministry of Health. 1998. Mortality 1998. Contexto Actual y Aspectos Relevantes. Mexico City, Ministry of Health.
-
- Ministry of Health. 2001. Mortality 2001. Contexto Actual y Aspectos Relevantes. Mexico City, Ministry of Health.
-
- Cahuana-Hurtado L, Sosa-Rubi S, Bertozzi S. Cost of mother-child care in Morelos State. Salud Publica Mex. 2004;46:316–25. - PubMed
-
- World Health Organization. Mother–baby package costing spreadsheet user guide. Geneva: World Health Organization; 1999.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
