

Different angiotensin-converting enzyme inhibitors have similar clinical efficacy after myocardial infarction
- PMID: 17711535
- PMCID: PMC2291228
- DOI: 10.1111/j.1365-2125.2007.02991.x
Different angiotensin-converting enzyme inhibitors have similar clinical efficacy after myocardial infarction
Abstract
What is already known about this subject: Treatment with an angiotensin-converting enzyme (ACE) inhibitor benefits many patients with cardiovascular disease. ACE inhibitors are generally assumed to be equally effective, but this has never been fully verified in clinical trials.
What this study adds: Studying the association among ACE inhibitors after myocardial infarction demonstrated similarity in clinical outcome and supports a dosage-response relationship. Therefore, for long-term benefits for patients who need treatment with an ACE inhibitor, a focus of treatment at the recommended dosage is most important and not which ACE inhibitor is used.
Aim: Therapy with angiotensin-converting enzyme (ACE) inhibitors is common after myocardial infarction (MI). Given the lack of randomized trials comparing different ACE inhibitors, the association among ACE inhibitors after MI in risk for mortality and reinfarction was studied.
Methods: Patients hospitalized with first-time MI (n = 16,068) between 1995 and 2002, who survived at least 30 days after discharge and claimed at least one prescription of ACE inhibitor, were identified using nationwide administrative registries in Denmark.
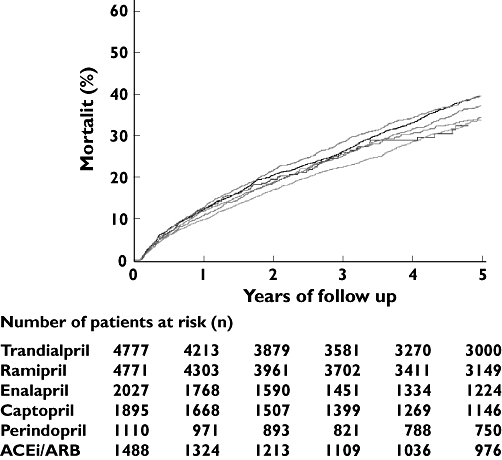
Results: Adjusted Cox regression analysis demonstrated no differences in risk for all-cause mortality, but patients using captopril had higher risk of reinfarction (hazard ratio 1.18, 95% confidence interval 1.05, 1.34). However, following adjustment for differences in used dosages, all ACE inhibitors had similar clinical efficacy. Risk of all-cause mortality: trandolapril (reference) 1.00, ramipril 0.97 (0.89, 1.05), enalapril 1.04 (0.95, 1.150), captopril 0.95 (0.83, 1.08), perindopril 0.98 (0.84, 1.15) and other ACE inhibitors or angiotensin II receptor blockers (ARB) 1.06 (0.94, 1.19). Reinfarction: trandolapril (reference) 1.00, ramipril 0.98 (0.89, 1.08), enalapril 1.04 (0.92, 1.17), captopril 1.05 (0.89, 1.25), perindopril 0.96 (0.81, 1.14) and other ACE inhibitors or ARB 0.99 (0.86, 1.14). Furthermore, the association between ARBs and clinical events was similar to ACE inhibitors (trandolapril reference): all-cause mortality 0.99 (0.84, 1.16) and recurrent MI 0.99 (0.83, 1.19).
Conclusions: Our results suggest a class effect among ACE inhibitors when used in comparable dosages. Focus on treatment at the recommended dosage is therefore most important, and not which ACE inhibitor is used.
Figures
References
-
- The Acute Infarction Ramipril Efficacy (AIRE) Study Investigators. Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. Lancet. 1993;342(8875):821–8. - PubMed
-
- Gruppo Italiano per lo Studio della Sopravvivenza nell'infarto Miocardico. GISSI-3: effects of lisinopril and transdermal glyceryl trinitrate singly and together on 6-week mortality and ventricular function after acute myocardial infarction. Lancet. 1994;343(8906):1115–22. - PubMed
-
- ISIS-4 (Fourth International Study of Infarct Survival) Collaborative Group. ISIS-4: a randomised factorial trial assessing early oral captopril, oral mononitrate, and intravenous magnesium sulphate in 58,050 patients with suspected acute myocardial infarction. Lancet. 1995;345(8951):669–85. - PubMed
-
- Pfeffer MA, Braunwald E, Moye LA, Basta L, Brown EJ, Jr, Cuddy TE, Davis BR, Geltman EM, Goldman S, Flaker GC. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med. 1992;327:669–77. - PubMed
-
- Kober L, Torp-Pedersen C, Carlsen JE, Bagger H, Eliasen P, Lyngborg K, Videbaek J, Cole DS, Auclert L, Pauly NC. A clinical trial of the angiotensin-converting-enzyme inhibitor trandolapril in patients with left ventricular dysfunction after myocardial infarction. Trandolapril Cardiac Evaluation (TRACE) Study Group. N Engl J Med. 1995;333:1670–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
