

Design of the Endobronchial Valve for Emphysema Palliation Trial (VENT): a non-surgical method of lung volume reduction
- PMID: 17711594
- PMCID: PMC1949836
- DOI: 10.1186/1471-2466-7-10
Design of the Endobronchial Valve for Emphysema Palliation Trial (VENT): a non-surgical method of lung volume reduction
Abstract
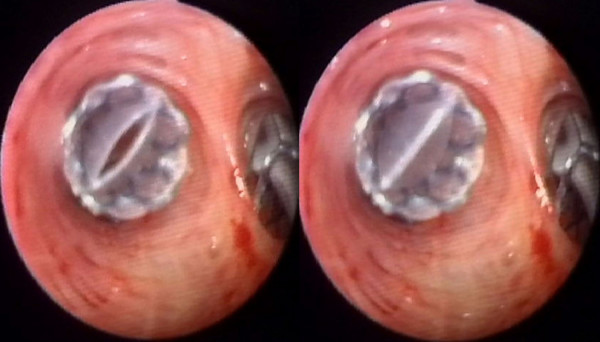
Background: Lung volume reduction surgery is effective at improving lung function, quality of life, and mortality in carefully selected individuals with advanced emphysema. Recently, less invasive bronchoscopic approaches have been designed to utilize these principles while avoiding the associated perioperative risks. The Endobronchial Valve for Emphysema PalliatioN Trial (VENT) posits that occlusion of a single pulmonary lobe through bronchoscopically placed Zephyr endobronchial valves will effect significant improvements in lung function and exercise tolerance with an acceptable risk profile in advanced emphysema.
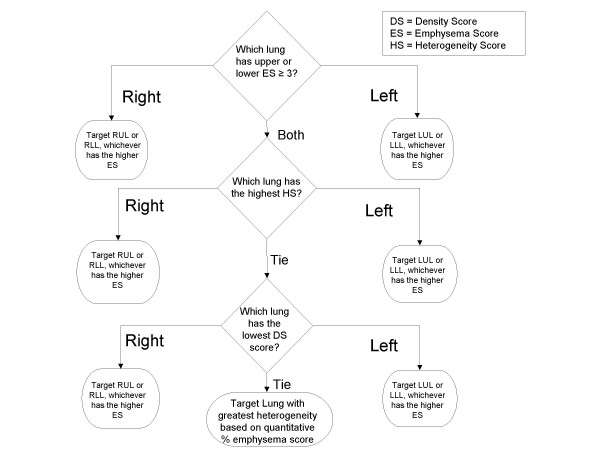
Methods: The trial design posted on Clinical trials.gov, on August 10, 2005 proposed an enrollment of 270 subjects. Inclusion criteria included: diagnosis of emphysema with forced expiratory volume in one second (FEV1) < 45% of predicted, hyperinflation (total lung capacity measured by body plethysmography > 100%; residual volume > 150% predicted), and heterogeneous emphysema defined using a quantitative chest computed tomography algorithm. Following standardized pulmonary rehabilitation, patients were randomized 2:1 to receive unilateral lobar placement of endobronchial valves plus optimal medical management or optimal medical management alone. The co-primary endpoint was the mean percent change in FEV1 and six minute walk distance at 180 days. Secondary end-points included mean percent change in St. George's Respiratory Questionnaire score and the mean absolute changes in the maximal work load measured by cycle ergometry, dyspnea (mMRC) score, and total oxygen use per day. Per patient response rates in clinically significant improvement/maintenance of FEV1 and six minute walk distance and technical success rates of valve placement were recorded. Apriori response predictors based on quantitative CT and lung physiology were defined.
Conclusion: If endobronchial valves improve FEV1 and health status with an acceptable safety profile in advanced emphysema, they would offer a novel intervention for this progressive and debilitating disease.
Trial registration: ClinicalTrials.gov: NCT00129584.
Figures

References
-
- Sciurba FC, Rogers RM, Keenan RJ, Slivka WA, Gorcsan J, 3rd, Ferson PF, Holbert JM, Brown ML, Landreneau RJ. Improvement in pulmonary function and elastic recoil after lung-reduction surgery for diffuse emphysema. The New England journal of medicine. 1996;334:1095–1099. doi: 10.1056/NEJM199604253341704. - DOI - PubMed
-
- Martinez FJ, de Oca MM, Whyte RI, Stetz J, Gay SE, Celli BR. Lung-volume reduction improves dyspnea, dynamic hyperinflation, and respiratory muscle function. American journal of respiratory and critical care medicine. 1997;155:1984–1990. - PubMed
-
- Sabanathan A, Sabanathan S, Shah R, Richardson J. Lung volume reduction surgery for emphysema. A review. The Journal of cardiovascular surgery. 1998;39:237–243. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
