

Repeated-slip training: an emerging paradigm for prevention of slip-related falls among older adults
- PMID: 17712033
- PMCID: PMC2826275
- DOI: 10.2522/ptj.20060326
Repeated-slip training: an emerging paradigm for prevention of slip-related falls among older adults
Abstract
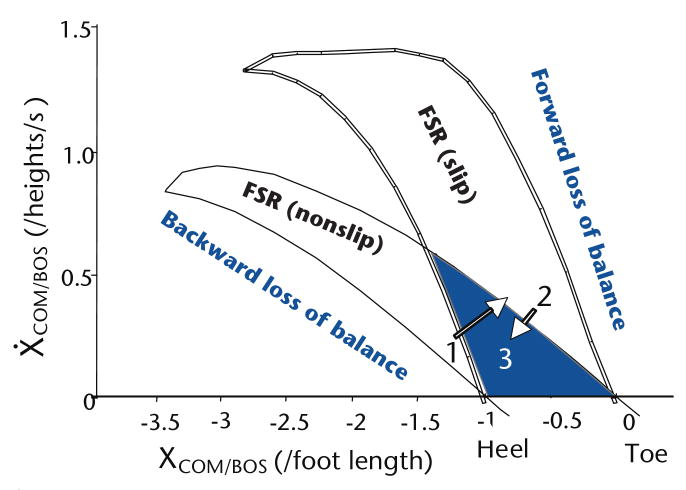
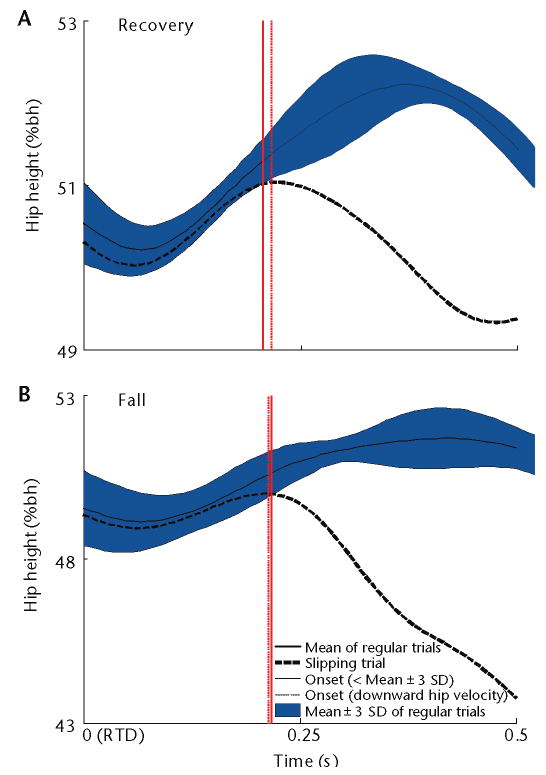
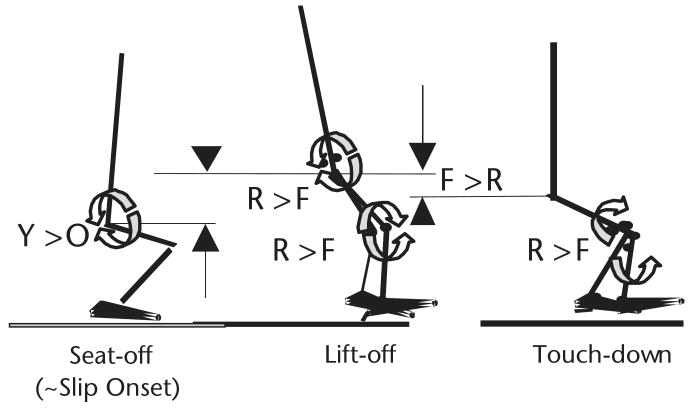
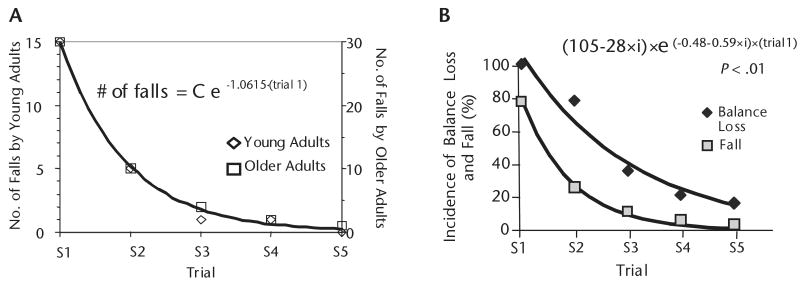
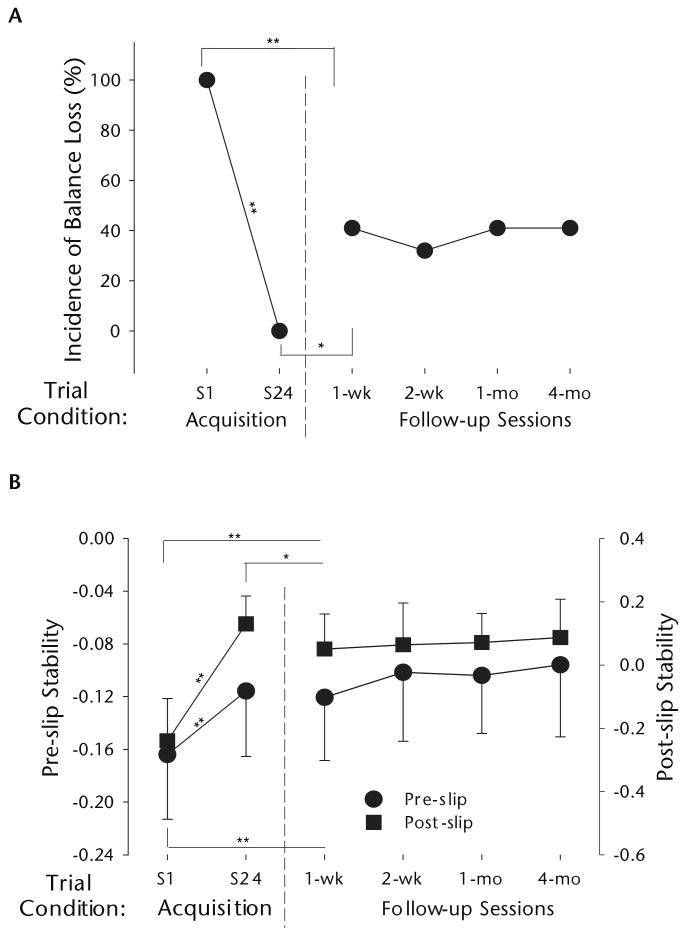
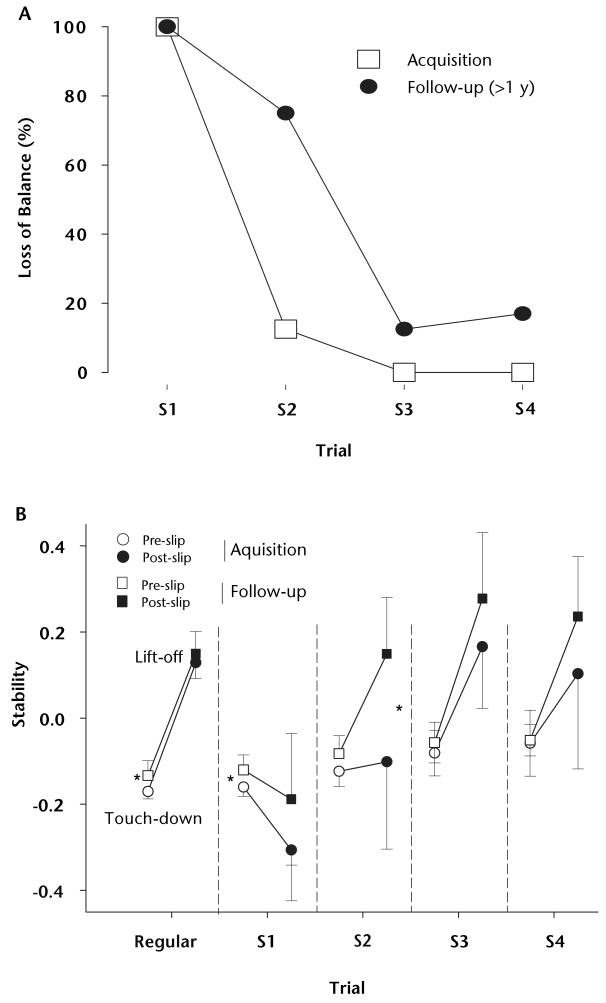
Falls frequently cause injury-related hospitalization or death among older adults. This article reviews a new conceptual framework on dynamic stability and weight support in reducing the risk for falls resulting from a forward slip, based on the principles of motor control and learning, in the context of adaptation and longer-term retention induced by repeated-slip training. Although an unexpected slip is severely destabilizing, a recovery step often is adequate for regaining stability, regardless of age. Consequently, poor weight support (quantified by reduction in hip height), rather than instability, is the major determinant of slip-related fall risk. Promisingly, a single session of repeated-slip training can enhance neuromechanical control of dynamic stability and weight support to prevent falls, which can be retained for several months or longer. These principles provide the theoretical basis for establishing task-specific adaptive training that facilitates the development of protective strategies to reduce falls among older adults.
Figures
Comment in
-
Invited commentary.Phys Ther. 2007 Nov;87(11):1491-3; author reply 1493-4. doi: 10.2522/ptj.20060326.ic. Phys Ther. 2007. PMID: 17974572 No abstract available.
References
-
- Rubenstein LZ, Josephson KR. The epidemiology of falls and syncope. Clin Geriatr Med. 2002;18:141–158. - PubMed
-
- Stelmach GE, Worringham CJ. Sensorimotor deficits related to postural stability: implications for falling in the elderly. Clin Geriatr Med. 1985;1:679–694. - PubMed
-
- Rubenstein LZ, Josephson KR, Robbins AS. Falls in the nursing home. Ann Intern Med. 1994;121:442–451. - PubMed
-
- Morley JE. A fall is a major event in the life of an older person. J Gerontol A Biol Sci Med Sci. 2002;57:M492–M495. - PubMed
-
- Baker SP, Harvey AH. Fall injuries in the elderly. Clin Geriatr Med. 1985;1:501–512. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
