

Clinical significance of the presence of amniotic fluid 'sludge' in asymptomatic patients at high risk for spontaneous preterm delivery
- PMID: 17712870
- PMCID: PMC2391008
- DOI: 10.1002/uog.4081
Clinical significance of the presence of amniotic fluid 'sludge' in asymptomatic patients at high risk for spontaneous preterm delivery
Abstract
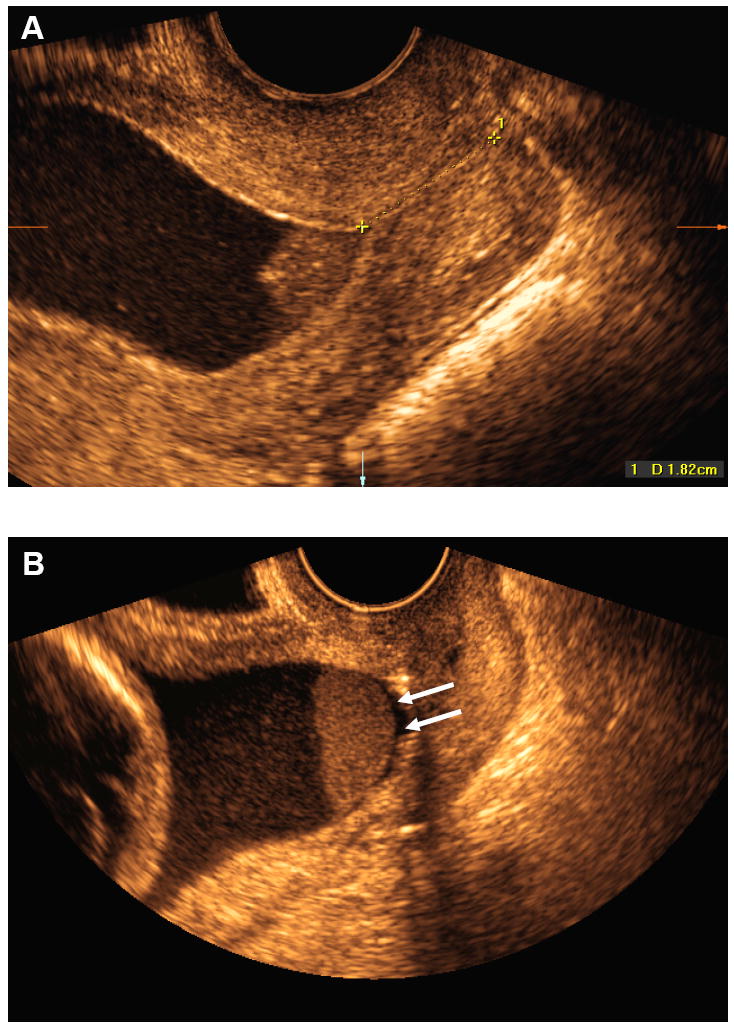
Objectives: To determine the clinical significance of the presence of amniotic fluid (AF) 'sludge' among asymptomatic patients at high risk for spontaneous preterm delivery.
Methods: This retrospective case-control study included 281 patients with (n = 66) or without (n = 215) AF 'sludge', who underwent transvaginal ultrasound examination between 13 and 29 completed weeks of gestation. Patients with threatened preterm labor, multiple gestation, fetal anomalies, placenta previa or uterine contractions were excluded.
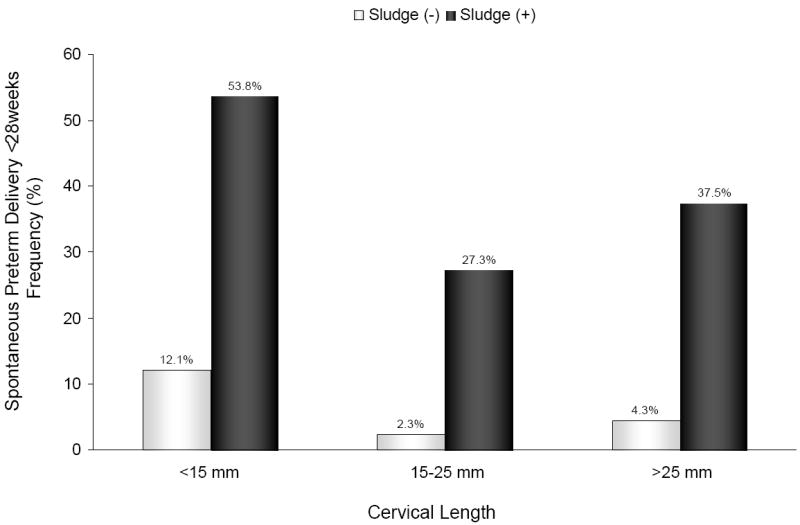
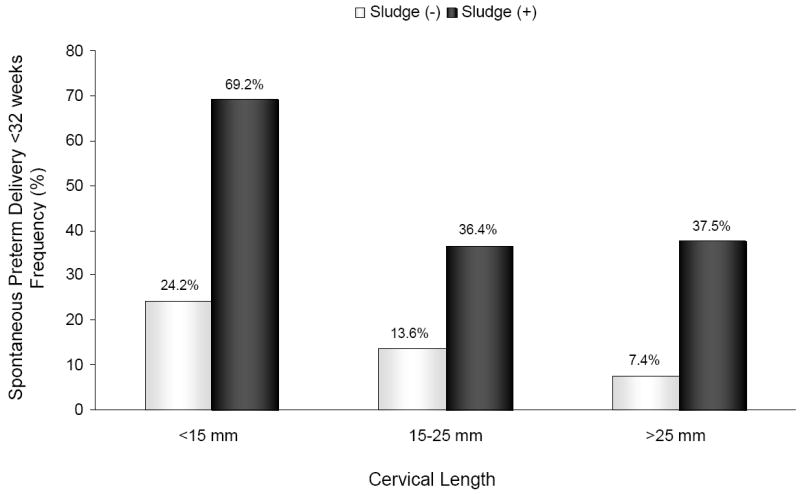
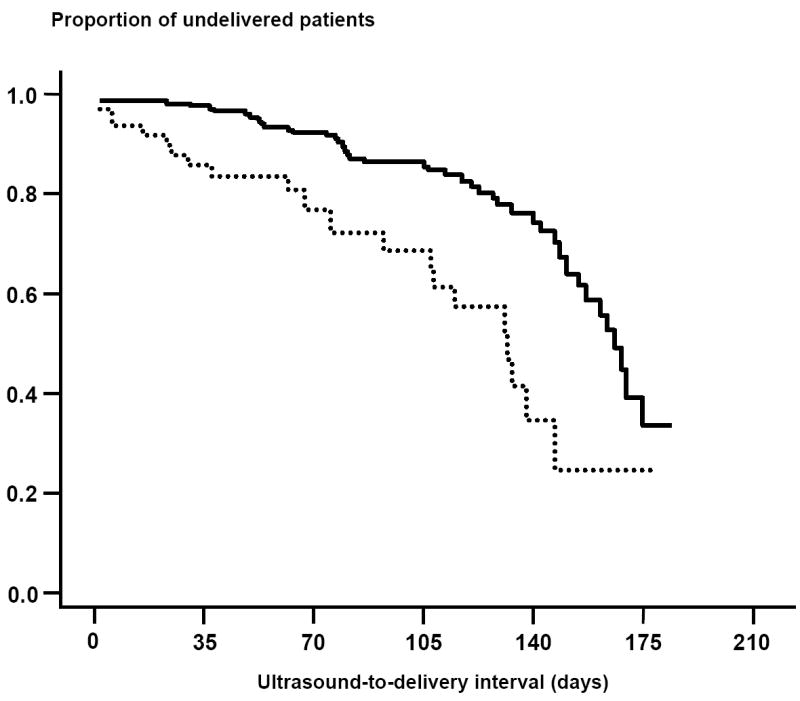
Results: The prevalence of AF 'sludge' in the study population was 23.5% (66/281). The rates of spontaneous preterm delivery at < 28 weeks, < 32 weeks, < 35 weeks and < 37 weeks of gestation were 14.7% (29/197), 21.3% (46/216), 28.7% (62/216) and 42.1% (91/216), respectively. Patients with 'sludge' had: (1) a higher rate of spontaneous preterm delivery at < 28 weeks (46.5% (20/43) vs. 5.8% (9/154); P < 0.001), < 32 weeks (55.6% (25/45) vs. 12.3% (21/171); P < 0.001) and < 35 weeks (62.2% (28/45) vs. 19.9% (34/171); P < 0.001); (2) a higher frequency of clinical chorioamnionitis (15.2% (10/66) vs. 5.1% (11/215); P = 0.007), histologic chorioamnionitis (61.5% (40/65) vs. 28% (54/193); P < 0.001) and funisitis (32.3% (21/65) vs. 19.2% (37/193); P = 0.03); (3) a higher frequency of preterm prelabor rupture of membranes (PROM) (39.4% (26/66) vs. 13.5% (29/215); P < 0.001), lower gestational age at preterm PROM (median 24.7 (interquartile range (IQR), 22.3-28.1) weeks vs. 32.3 (IQR, 27.7-34.8) weeks; P < 0.001); and (4) shorter median ultrasound-to-delivery interval ('sludge' positive 127 days (95% CI, 120-134 days) vs. 'sludge' negative 161 days (95% CI, 153-169 days); P < 0.001) and ultrasound-to-preterm PROM interval ('sludge' positive 23 days (95% CI, 7-39 days) vs. 'sludge' negative 57 days (95% CI, 38-77 days); P = 0.003) than those without 'sludge'. AF 'sludge' was an independent explanatory variable for the occurrence of spontaneous preterm delivery at < 28 weeks, < 32 weeks and < 35 weeks, preterm PROM, microbial invasion of the amniotic cavity (MIAC) and histologic chorioamnionitis. Moreover, the combination of a cervical length < 25 mm and 'sludge' conferred an odds ratio of 14.8 and 9.9 for spontaneous preterm delivery at < 28 weeks and < 32 weeks, respectively.
Conclusions: AF 'sludge' is an independent risk factor for spontaneous preterm delivery, preterm PROM, MIAC and histologic chorioamnionitis in asymptomatic patients at high risk for spontaneous preterm delivery. Furthermore, the combination of 'sludge' and a short cervix confers a higher risk for spontaneous preterm delivery at < 28 weeks and < 32 weeks than a short cervix alone.
Copyright (c) 2007 ISUOG
Figures
References
-
- Espinoza J, Goncalves LF, Romero R, Nien JK, Stites S, Kim YM, et al. The prevalence and clinical significance of amniotic fluid ‘sludge’ in patients with preterm labor and intact membranes. Ultrasound Obstet Gynecol. 2005;25:346–52. - PubMed
-
- Bujold E, Pasquier JC, Simoneau J, Arpin MH, Duperron L, Morency AM, et al. Intra-amniotic sludge, short cervix, and risk of preterm delivery. J Obstet Gynaecol Can. 2006;28:198–202. - PubMed
-
- Cassell GH, Davis RO, Waites KB, Brown MB, Marriott PA, Stagno S, et al. Isolation of Mycoplasma hominis and Ureaplasma urealyticum from amniotic fluid at 16-20 weeks of gestation: potential effect on outcome of pregnancy. Sex Transm Dis. 1983;10:294–302. - PubMed
-
- Gray DJ, Robinson HB, Malone J, Thomson RB., Jr Adverse outcome in pregnancy following amniotic fluid isolation of Ureaplasma urealyticum. Prenat Diagn. 1992;12:111–17. - PubMed
-
- Horowitz S, Mazor M, Romero R, Horowitz J, Glezerman M. Infection of the amniotic cavity with Ureaplasma urealyticum in the midtrimester of pregnancy. J Reprod Med. 1995;40:375–79. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
