

Burn size determines the inflammatory and hypermetabolic response
- PMID: 17716366
- PMCID: PMC2206482
- DOI: 10.1186/cc6102
Burn size determines the inflammatory and hypermetabolic response
Abstract
Background: Increased burn size leads to increased mortality of burned patients. Whether mortality is due to inflammation, hypermetabolism or other pathophysiologic contributing factors is not entirely determined. The purpose of the present study was to determine in a large prospective clinical trial whether different burn sizes are associated with differences in inflammation, body composition, protein synthesis, or organ function.
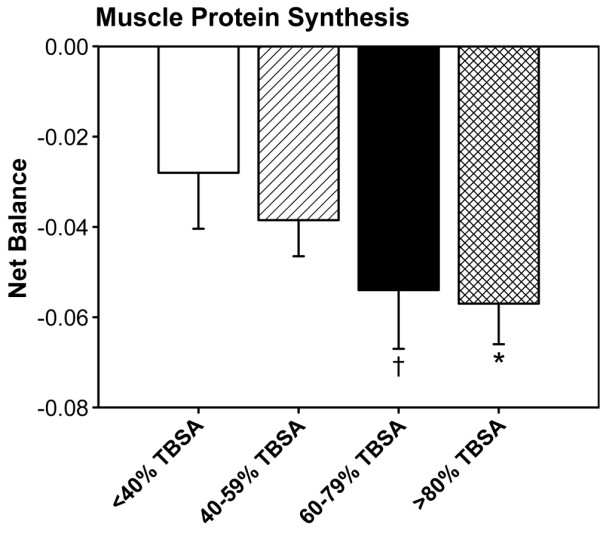
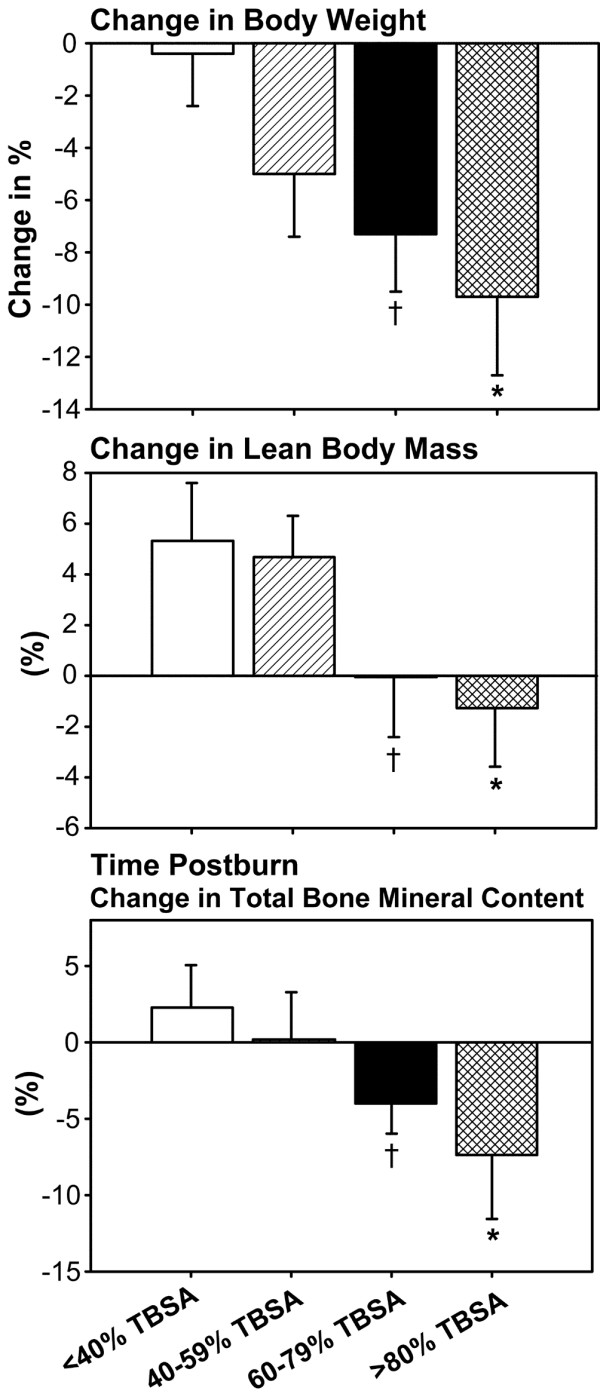
Methods: Pediatric burned patients were divided into four burn size groups: <40% total body surface area (TBSA) burn, 40-59% TBSA burn, 60-79% TBSA burn, and >80% TBSA burn. Demographic and clinical data, hypermetabolism, the inflammatory response, body composition, the muscle protein net balance, serum and urine hormones and proteins, and cardiac function and changes in liver size were determined.
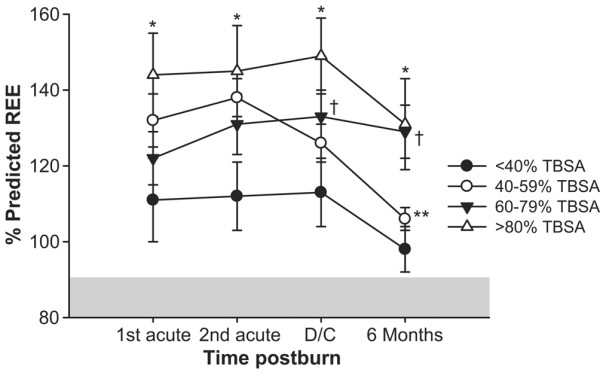
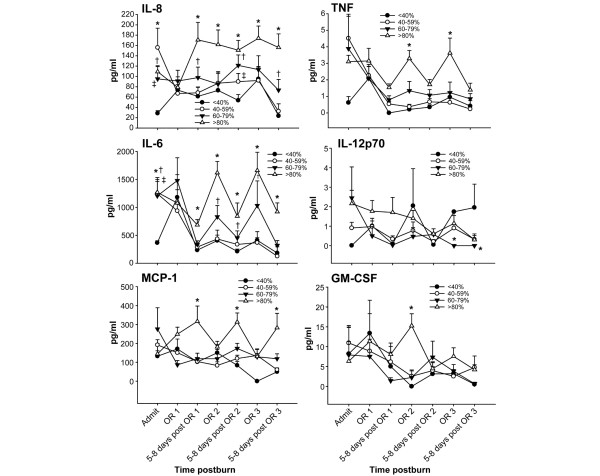
Results: One hundred and eighty-nine pediatric patients of similar age and gender distribution were included in the study (<40% TBSA burn, n = 43; 40-59% TBSA burn, n = 79; 60-79% TBSA burn, n = 46; >80% TBSA burn, n = 21). Patients with larger burns had more operations, a greater incidence of infections and sepsis, and higher mortality rates compared with the other groups (P < 0.05). The percentage predicted resting energy expenditure was highest in the >80% TBSA group, followed by the 60-79% TBSA burn group (P < 0.05). Children with >80% burns lost the most body weight, lean body mass, muscle protein and bone mineral content (P < 0.05). The urine cortisol concentration was highest in the 80-99% and 60-79% TBSA burn groups, associated with significant myocardial depression and increased change in liver size (P < 0.05). The cytokine profile showed distinct differences in expression of IL-8, TNF, IL-6, IL-12p70, monocyte chemoattractant protein-1 and granulocyte-macrophage colony-stimulating factor (P < 0.05).
Conclusion: Morbidity and mortality in burned patients is burn size dependent, starts at a 60% TBSA burn and is due to an increased hypermetabolic and inflammatory reaction, along with impaired cardiac function.
Figures



References
-
- Przkora R, Barrow RE, Jeschke MG, Suman OE, Celis M, Sanford AP, Chinkes DL, Mlcak RP, Herndon DN. Body composition changes with time in pediatric burn patients. J Trauma. 2006;60:968–971. - PubMed
-
- Rennie MJ. Muscle protein turnover and the wasting due to injury and disease. Br Med Bull. 1985;41:257–264. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
