

The effect of oxandrolone on the endocrinologic, inflammatory, and hypermetabolic responses during the acute phase postburn
- PMID: 17717439
- PMCID: PMC1959346
- DOI: 10.1097/SLA.0b013e318146980e
The effect of oxandrolone on the endocrinologic, inflammatory, and hypermetabolic responses during the acute phase postburn
Abstract
Objective and summary background data: Postburn long-term oxandrolone treatment improves hypermetabolism and body composition. The effects of oxandrolone on clinical outcome, body composition, endocrine system, and inflammation during the acute phase postburn in a large prospective randomized single-center trial have not been studied.
Methods: Burned children (n = 235) with >40% total body surface area burn were randomized (block randomization 4:1) to receive standard burn care (control, n = 190) or standard burn care plus oxandrolone for at least 7 days (oxandrolone 0.1 mg/kg body weight q.12 hours p.o, n = 45). Clinical parameters, body composition, serum hormones, and cytokine expression profiles were measured throughout acute hospitalization. Statistical analysis was performed by Student t test, or ANOVA followed by Bonferroni correction with significance accepted at P < 0.05.
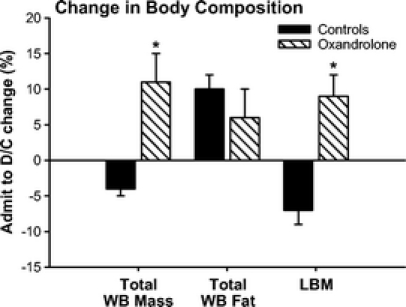
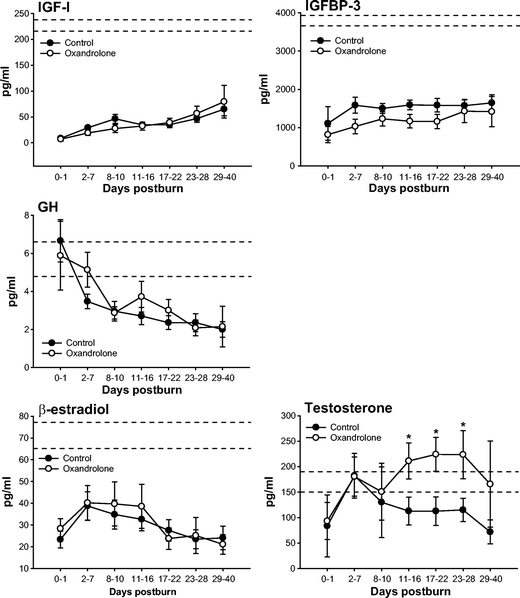
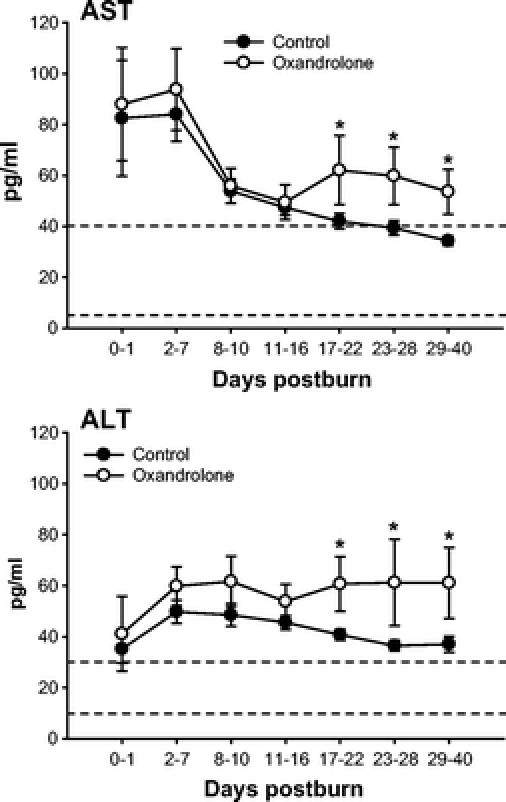
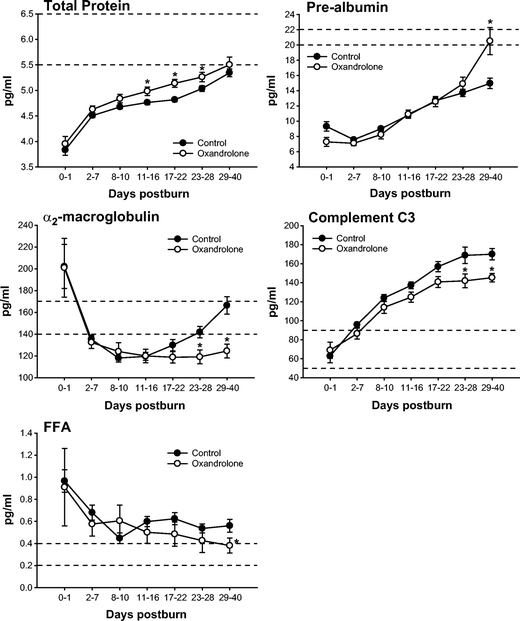
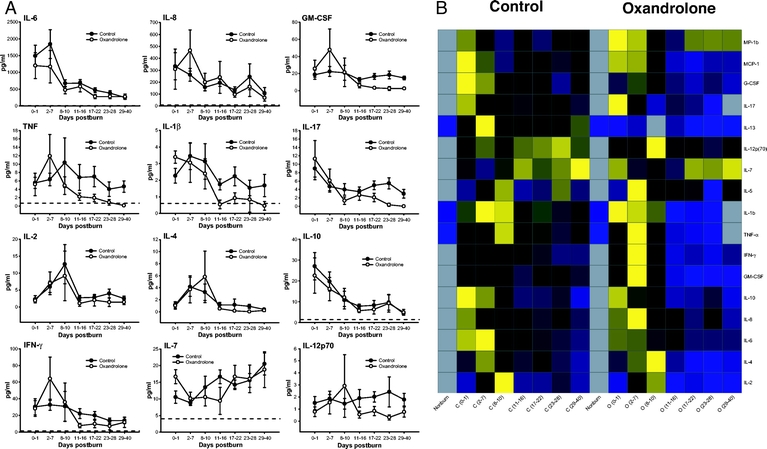
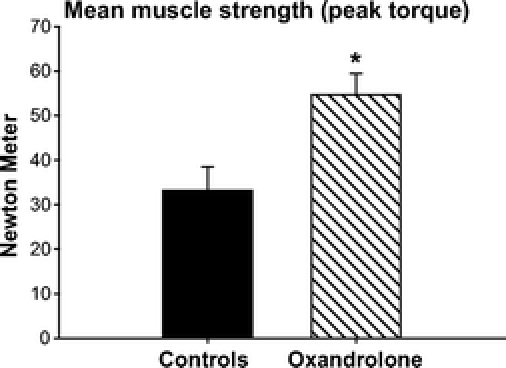
Results: Demographics and clinical data were similar in both groups. Length of intensive care unit stay was significantly decreased in oxandrolone-treated patients (0.48 +/- 0.02 days/% burn) compared with controls (0.56 +/- 0.02 days/% burn), (P < 0.05). Control patients lost 8 +/- 1% of their lean body mass (LBM), whereas oxandrolone-treated patients had preserved LBM (+9 +/- 4%), P < 0.05. Oxandrolone significantly increased serum prealbumin, total protein, testosterone, and AST/ALT, whereas it significantly decreased alpha2-macroglobulin and complement C3, P < 0.05. Oxandrolone did not adversely affect the endocrine and inflammatory response as we found no significant differences in the hormone panels and cytokine expression profiles.
Conclusions: In this large prospective, double-blinded, randomized single-center study, oxandrolone shortened length of acute hospital stay, maintained LBM, improved body composition and hepatic protein synthesis while having no adverse effects on the endocrine axis postburn, but was associated with an increase in AST and ALT.
Figures
Similar articles
-
Metabolic and hormonal changes of severely burned children receiving long-term oxandrolone treatment.Ann Surg. 2005 Sep;242(3):384-9, discussion 390-1. doi: 10.1097/01.sla.0000180398.70103.24. Ann Surg. 2005. PMID: 16135924 Free PMC article. Clinical Trial.
-
Five-year outcomes after oxandrolone administration in severely burned children: a randomized clinical trial of safety and efficacy.J Am Coll Surg. 2012 Apr;214(4):489-502; discussion 502-4. doi: 10.1016/j.jamcollsurg.2011.12.038. J Am Coll Surg. 2012. PMID: 22463890 Free PMC article. Clinical Trial.
-
Improved net protein balance, lean mass, and gene expression changes with oxandrolone treatment in the severely burned.Ann Surg. 2003 Jun;237(6):801-10; discussion 810-1. doi: 10.1097/01.SLA.0000071562.12637.3E. Ann Surg. 2003. PMID: 12796576 Free PMC article. Clinical Trial.
-
Oxandrolone in pediatric patients with severe thermal burn injury.Ann Pharmacother. 2008 Sep;42(9):1310-5. doi: 10.1345/aph.1L162. Epub 2008 Aug 5. Ann Pharmacother. 2008. PMID: 18682543 Review.
-
Oxandrolone treatment in adults with severe thermal injury.Pharmacotherapy. 2009 Feb;29(2):213-26. doi: 10.1592/phco.29.2.213. Pharmacotherapy. 2009. PMID: 19170590 Review.
Cited by
-
Predictive Value of IL-8 for Sepsis and Severe Infections After Burn Injury: A Clinical Study.Shock. 2015 Mar;43(3):222-7. doi: 10.1097/SHK.0000000000000294. Shock. 2015. PMID: 25514427 Free PMC article. Clinical Trial.
-
The P50 Research Center in Perioperative Sciences: How the investment by the National Institute of General Medical Sciences in team science has reduced postburn mortality.J Trauma Acute Care Surg. 2017 Sep;83(3):532-542. doi: 10.1097/TA.0000000000001644. J Trauma Acute Care Surg. 2017. PMID: 28697015 Free PMC article.
-
Update on Hypermetabolism in Pediatric Burn Patients.Semin Plast Surg. 2024 Apr 4;38(2):133-144. doi: 10.1055/s-0044-1782649. eCollection 2024 May. Semin Plast Surg. 2024. PMID: 38746705 Free PMC article. Review.
-
Hormone treatment and muscle anabolism during aging: androgens.Clin Nutr. 2010 Dec;29(6):697-700. doi: 10.1016/j.clnu.2010.03.010. Epub 2010 May 7. Clin Nutr. 2010. PMID: 20452103 Free PMC article. Review.
-
What, how, and how much should patients with burns be fed?Surg Clin North Am. 2011 Jun;91(3):609-29. doi: 10.1016/j.suc.2011.03.002. Surg Clin North Am. 2011. PMID: 21621699 Free PMC article. Review.
References
-
- Finnerty CC, Herndon DN, Przkora R, et al. Cytokine expression profile over time in severely burned pediatric patients. Shock. 2006;26:13–19. - PubMed
-
- Herndon DN, Tompkins RG. Support of the metabolic response to burn injury. Lancet. 2004;363:1895–1902. - PubMed
-
- Wilmore DW, Aulick LH. Metabolic changes in burned patients. Surg Clin North Am. 1978;58:1173–1187. - PubMed
-
- Hasselgren PO. Glucocorticoids and muscle catabolism. Curr Opin Clin Nutr Metab Care. 1999;2:201–205. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
