

Two thousand transhiatal esophagectomies: changing trends, lessons learned
- PMID: 17717440
- PMCID: PMC1959358
- DOI: 10.1097/SLA.0b013e31814697f2
Two thousand transhiatal esophagectomies: changing trends, lessons learned
Abstract
Objective: "Rediscovered" in 1976, transhiatal esophagectomy (THE) has been applicable in most situations requiring esophageal resection and reconstruction. The objective of this study was to review the authors' 30-year experience with THE and changing trends in its use.
Methods: Using the authors' prospective Esophagectomy Database, this single institution experience with THE was analyzed retrospectively.
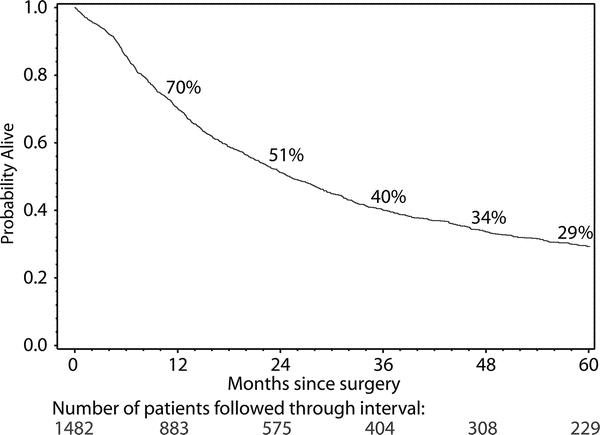
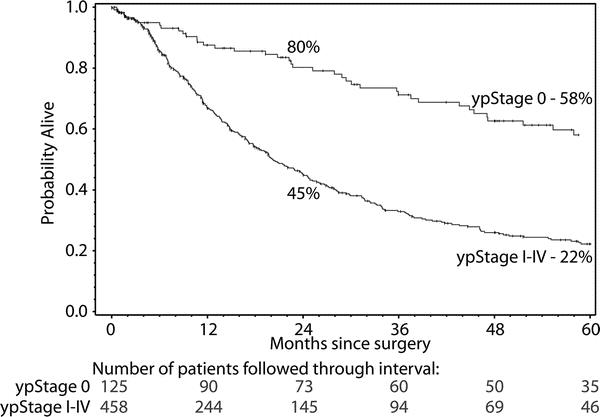
Results: Two thousand and seven THEs were performed-1063 (previously reported) between 1976 and 1998 (group I) and 944 from 1998 to 2006 (group II), 24% for benign disease, 76%, cancer. THE was possible in 98%. Stomach was the esophageal substitute in 97%. Comparing outcomes between group I and group II, statistically significant differences (P < 0.001) were observed in hospital mortality (4% vs. 1%); adenocarcinoma histology (69% vs. 86%); use of neoadjuvant chemoradiation (28% vs. 52%); mean blood loss (677 vs. 368 mL); anastomotic leak (14% vs. 9%); and discharge within 10 days (52% vs. 78%). Major complications remain infrequent: wound infection/dehiscence, 3%, atelectasis/pneumonia, 2%, intrathoracic hemorrhage, recurrent laryngeal nerve paralysis, chylothorax, and tracheal laceration, <1% each. Late functional results have been good or excellent in 73%. Aggressive preoperative conditioning, avoiding the ICU, improved pain management, and early ambulation reduce length of stay, with 50% in group II discharged within 1 week.
Conclusion: THE refinements have reduced the historic morbidity and mortality of esophageal resection. This largest reported THE experience reinforces the value of consistent technique and a clinical pathway in managing these high acuity esophageal patients.
Figures



References
-
- Orringer MB, Sloan H. Esophagectomy without thoracotomy. J Thorac Cardiovasc Surg. 1978;76:643–654. - PubMed
-
- Denk W. Zur Radikaloperation des Osophaguskarfzentralbl. Chirurg. 1913;40:1065–1068.
-
- Turner GG. Excision of thoracic esophagus for carcinoma with construction of extrathoracic gullet. Lancet. 1933;2:1315–1316.
-
- Ong GB, Lee TC. Pharyngogastric anastomosis after oesophagopharyngectomy for carcinoma of the hypopharynx and cervical oesophagus. Br J Surg. 1960;48:193–200. - PubMed
-
- LeQuesne LP, Ranger D. Pharyngogastrectomy with immediate pharyngogastric anastomosis. Br J Surg. 1966;53:105–109. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
