

Extent of surgery affects survival for papillary thyroid cancer
- PMID: 17717441
- PMCID: PMC1959355
- DOI: 10.1097/SLA.0b013e31814697d9
Extent of surgery affects survival for papillary thyroid cancer
Abstract
Background: The extent of surgery for papillary thyroid cancers (PTC) remains controversial. Consensus guidelines have recommended total thyroidectomy for PTC > or =1 cm; however, no study has supported this recommendation based on a survival advantage. The objective of this study was to examine whether the extent of surgery affects outcomes for PTC and to determine whether a size threshold could be identified above which total thyroidectomy is associated with improved outcomes.
Methods: From the National Cancer Data Base (1985-1998), 52,173 patients underwent surgery for PTC. Survival was estimated by the Kaplan-Meier method and compared using log-rank tests. Cox Proportional Hazards modeling stratified by tumor size was used to assess the impact of surgical extent on outcomes and to identify a tumor size threshold above which total thyroidectomy is associated with an improvement in recurrence and long-term survival rates.
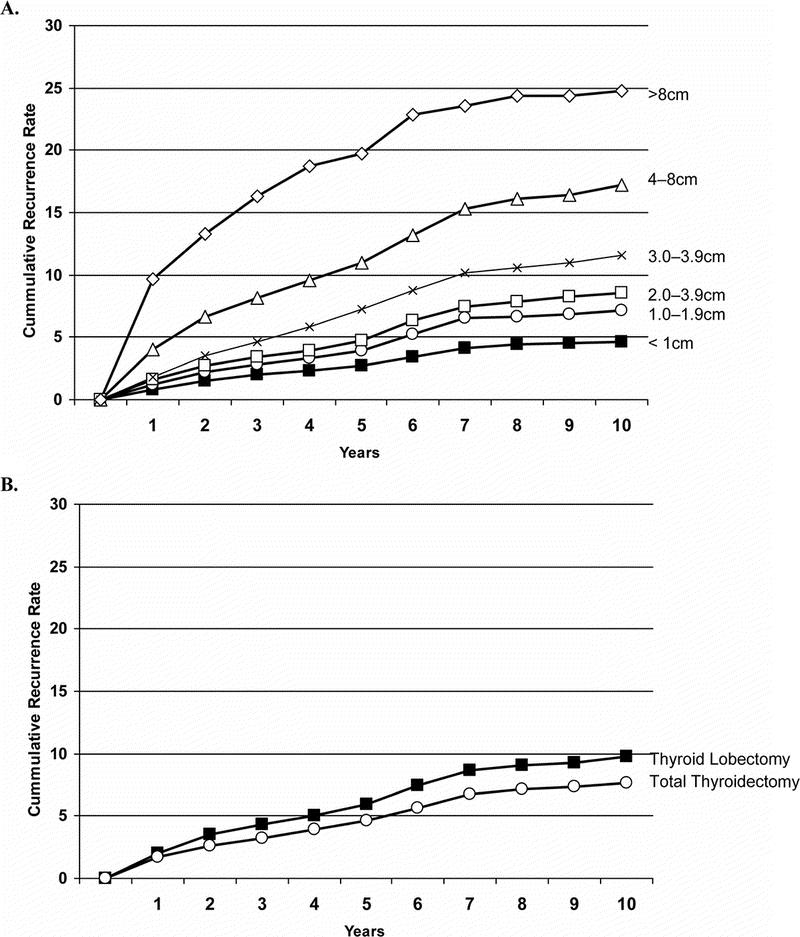
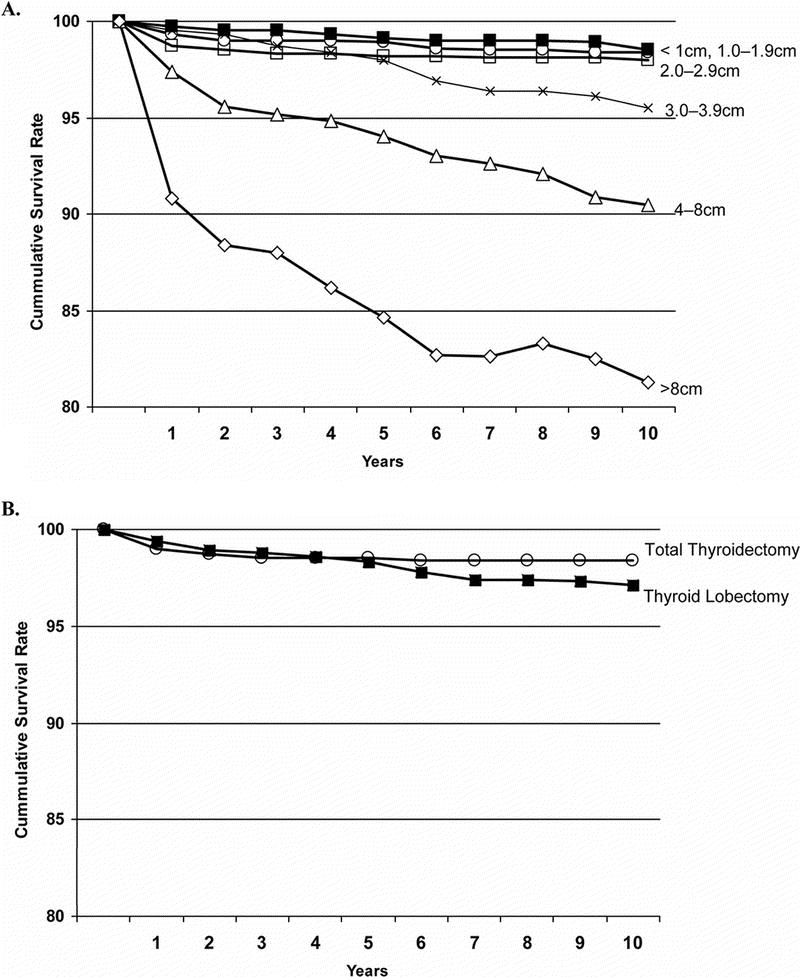
Results: Of the 52,173 patients, 43,227 (82.9%) underwent total thyroidectomy, and 8946 (17.1%) underwent lobectomy. For PTC <1 cm extent of surgery did not impact recurrence or survival (P = 0.24, P = 0.83). For tumors > or =1 cm, lobectomy resulted in higher risk of recurrence and death (P = 0.04, P = 0.009). To minimize the influence of larger tumors, 1 to 2 cm lesions were examined separately: lobectomy again resulted in a higher risk of recurrence and death (P = 0.04, P = 0.04).
Conclusions: The results of this study demonstrate that total thyroidectomy results in lower recurrence rates and improved survival for PTC > or =1.0 cm compared with lobectomy. This is the first study to demonstrate that total thyroidectomy for PTC > or =1.0 cm improves outcomes.
Figures
Comment in
-
Is total thyroidectomy the procedure of choice for papillary thyroid cancer?Nat Clin Pract Oncol. 2008 Apr;5(4):184-5. doi: 10.1038/ncponc1067. Epub 2008 Feb 5. Nat Clin Pract Oncol. 2008. PMID: 18253103 No abstract available.
-
Re: Extent of surgery affects papillary thyroid cancer.Ann Surg. 2008 Jun;247(6):1082-3; author reply 1083-4. doi: 10.1097/SLA.0b013e3181758d93. Ann Surg. 2008. PMID: 18520248 No abstract available.
-
Extent of surgery affects papillary thyroid cancer.Ann Surg. 2009 Mar;249(3):549-50; author reply 550. doi: 10.1097/SLA.0b013e31819ac700. Ann Surg. 2009. PMID: 19247059 No abstract available.
References
-
- American Cancer Society. Cancer facts and figures. Available at: www.cancer.org/docroot/STT/content/STT_1x_Cancer_Facts_Figures_2007.asp. Accessed January 21, 2007.
-
- Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973–2002. JAMA. 2006;295:2164–2167. - PubMed
-
- Hodgson NC, Button J, Solorzano CC. Thyroid cancer: is the incidence still increasing? Ann Surg Oncol. 2004;11:1093–1097. - PubMed
-
- Mazzaferri EL. Managing small thyroid cancers. JAMA. 2006;295:2179–2182. - PubMed
-
- Kebebew E, Clark OH. Differentiated thyroid cancer: “complete” rational approach. World J Surg. 2000;24:942–951. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
