

Shifting paradigms in the treatment of lower extremity vascular disease: a report of 1000 percutaneous interventions
- PMID: 17717445
- PMCID: PMC1959357
- DOI: 10.1097/SLA.0b013e31814699a2
Shifting paradigms in the treatment of lower extremity vascular disease: a report of 1000 percutaneous interventions
Abstract
Objectives: Catheter-based revascularization has emerged as an alternative to surgical bypass for lower extremity vascular disease and is a frequently used tool in the armamentarium of the vascular surgeon. In this study we report contemporary outcomes of 1000 percutaneous infra-inguinal interventions performed by a single vascular surgery division.
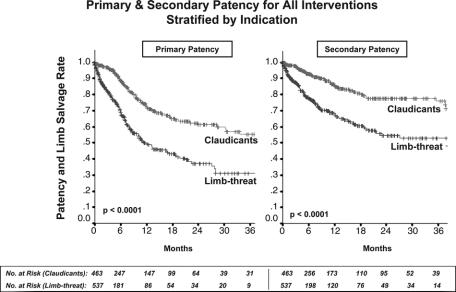
Methods: We evaluated a prospectively maintained database of 1000 consecutive percutaneous infra-inguinal interventions between 2001 and 2006 performed for claudication (46.3%) or limb-threatening ischemia (52.7%; rest pain in 27.7% and tissue loss in 72.3%). Treatments included angioplasty with or without stenting, laser angioplasty, and atherectomy of the femoral, popliteal, and tibial vessels.
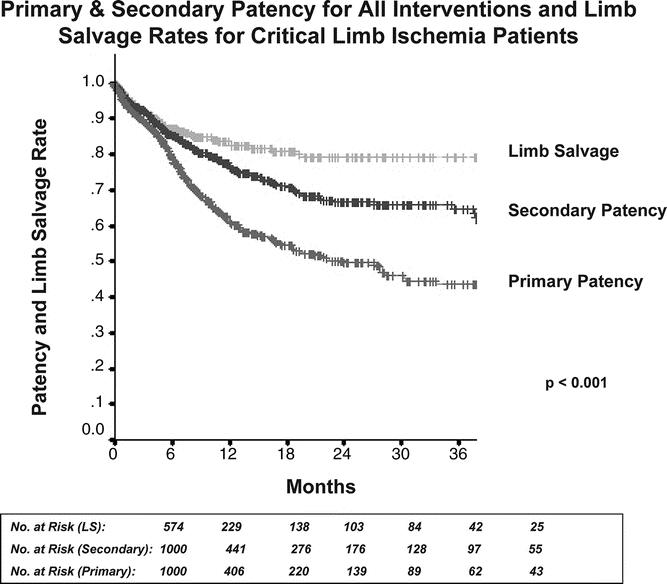
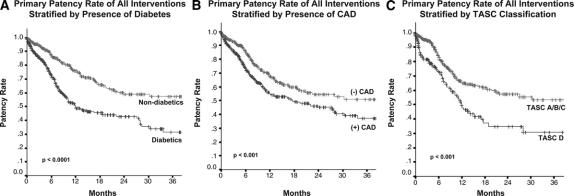
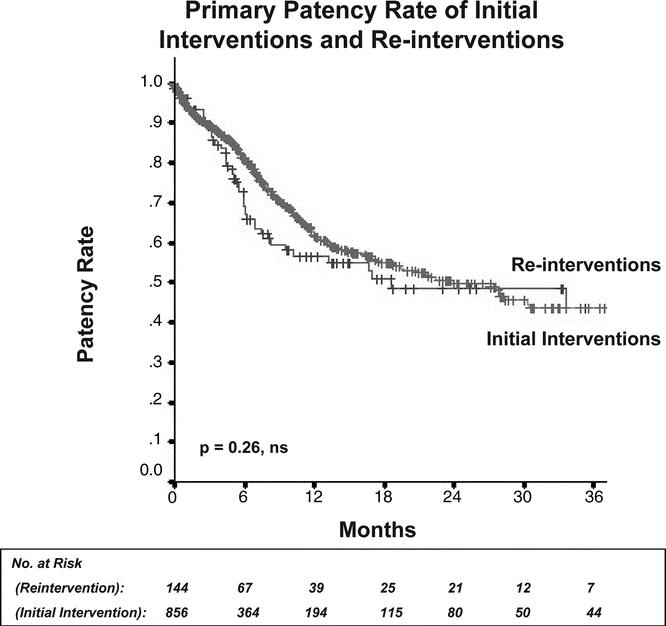
Results: Mean age was 71.4 years and 57.3% were male; comorbidities included hypertension (84%), coronary artery disease (51%), diabetes (58%), tobacco use (52%), and chronic renal insufficiency (39%). Overall 30-day mortality was 0.5%. Two-year primary and secondary patencies and rate of amputation were 62.4%, 79.3%, and 0.5%, respectively, for patients with claudication. Two-year primary and secondary patencies and limb salvage rates were 37.4%, 55.4%, and 79.3% for patients with limb-threatening ischemia. By multivariable Cox PH modeling, limb-threat as procedural indication (P < 0.0001), diabetes (P = 0.003), hypercholesterolemia (P = 0.001), coronary artery disease (P = 0.047), and Transatlantic Inter-Society Consensus D lesion complexity (P = 0.050) were independent predictors of recurrent disease. For patients that developed recurrent disease, 7.5% required no further intervention, 60.3% underwent successful percutaneous reintervention, 11.7% underwent bypass and 20.5% underwent amputation. Patency rates were identical for the initial procedure and subsequent reinterventions (P = 0.97).
Conclusion: Percutaneous therapy for peripheral vascular disease is associated with minimal mortality and can achieve 2-year secondary patency rates of nearly 80% in patients with claudication. Although patency is diminished in patients with limb-threat, limb-salvage rates remain reasonable at close to 80% at 2 years. Percutaneous infra-inguinal revascularization carries a low risk of morbidity and mortality, and should be considered first-line therapy in patients with chronic lower extremity ischemia.
Figures
Similar articles
-
Lesion severity and treatment complexity are associated with outcome after percutaneous infra-inguinal intervention.J Vasc Surg. 2007 Oct;46(4):709-16. doi: 10.1016/j.jvs.2007.05.059. J Vasc Surg. 2007. PMID: 17903651
-
Femoral artery percutaneous revascularization for patients with critical limb ischemia: outcomes compared to patients with claudication over 2.5 years.Vasc Med. 2012 Jun;17(3):138-44. doi: 10.1177/1358863X12440141. Epub 2012 Apr 11. Vasc Med. 2012. PMID: 22496125
-
Reduced primary patency rate in diabetic patients after percutaneous intervention results from more frequent presentation with limb-threatening ischemia.J Vasc Surg. 2008 Jan;47(1):101-8. doi: 10.1016/j.jvs.2007.09.018. J Vasc Surg. 2008. PMID: 18178459
-
Medical and endovascular management of critical limb ischemia.J Endovasc Ther. 2009 Apr;16(2 Suppl 2):II31-62. doi: 10.1583/08-2657.1. J Endovasc Ther. 2009. PMID: 19624074 Review.
-
The natural history of peripheral vascular disease. Implications for its management.Circulation. 1991 Feb;83(2 Suppl):I12-9. Circulation. 1991. PMID: 1991393 Review.
Cited by
-
Magnetic resonance imaging-based computational modelling of blood flow and nanomedicine deposition in patients with peripheral arterial disease.J R Soc Interface. 2015 May 6;12(106):20150001. doi: 10.1098/rsif.2015.0001. J R Soc Interface. 2015. PMID: 25878124 Free PMC article. Clinical Trial.
-
Predictors of failure and success of tibial interventions for critical limb ischemia.J Vasc Surg. 2010 Oct;52(4):834-42. doi: 10.1016/j.jvs.2010.04.070. J Vasc Surg. 2010. PMID: 20619586 Free PMC article.
-
Multilevel versus isolated endovascular tibial interventions for critical limb ischemia.J Vasc Surg. 2011 Sep;54(3):722-9. doi: 10.1016/j.jvs.2011.03.232. Epub 2011 Jul 30. J Vasc Surg. 2011. PMID: 21803523 Free PMC article.
-
Endovascular recanalization of chronic total occlusions of the native superficial femoral artery after failed femoropopliteal bypass in patients with critical limb ischemia.CVIR Endovasc. 2021 Sep 7;4(1):68. doi: 10.1186/s42155-021-00256-0. CVIR Endovasc. 2021. PMID: 34491477 Free PMC article.
-
Non-Surgical treatment Versus Surgery for Iatrogenic Femoral Artery Pseudoaneurysms: Systematic Review and Meta-Analysis.Front Surg. 2022 Jun 8;9:905701. doi: 10.3389/fsurg.2022.905701. eCollection 2022. Front Surg. 2022. PMID: 36211300 Free PMC article. Review.
References
-
- Hackam DG. Cardiovascular risk prevention in peripheral artery disease. J Vasc Surg. 2005;41:1070–1073. - PubMed
-
- Yeager RA, Moneta GL, Taylor LM Jr, et al. Surgical management of severe acute lower extremity ischemia. J Vasc Surg. 1992;15:385–391; discussion 392–393. - PubMed
-
- Hunink MG, Wong JB, Donaldson MC, et al. Revascularization for femoropopliteal disease. A decision and cost-effectiveness analysis. JAMA. 1995;274:165–171. - PubMed
-
- Garcia LA. Epidemiology and pathophysiology of lower extremity peripheral arterial disease. J Endovasc Ther. 2006;13:II3–II9. - PubMed
-
- Ouriel K. Peripheral arterial disease. Lancet. 2001;358:1257–1264. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
