

Seasonal variation in surgical outcomes as measured by the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP)
- PMID: 17717449
- PMCID: PMC1959349
- DOI: 10.1097/SLA.0b013e31814855f2
Seasonal variation in surgical outcomes as measured by the American College of Surgeons-National Surgical Quality Improvement Program (ACS-NSQIP)
Abstract
Objective: We hypothesize that the systems of care within academic medical centers are sufficiently disrupted with the beginning of a new academic year to affect patient outcomes.
Methods: This observational multiinstitutional cohort study was conducted by analysis of the National Surgical Quality Improvement Program-Patient Safety in Surgery Study database. The 30-day morbidity and mortality rates were compared between 2 periods of care: (early group: July 1 to August 30) and late group (April 15 to June 15). Patient baseline characteristics were first compared between the early and late periods. A prediction model was then constructed, via stepwise logistic regression model with a significance level for entry and a significance level for selection of 0.05.
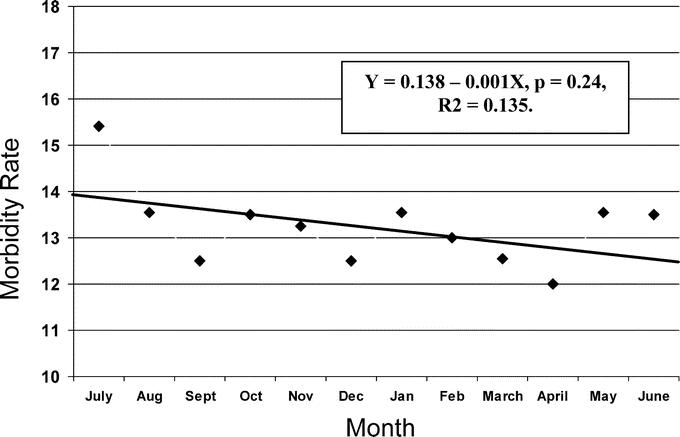
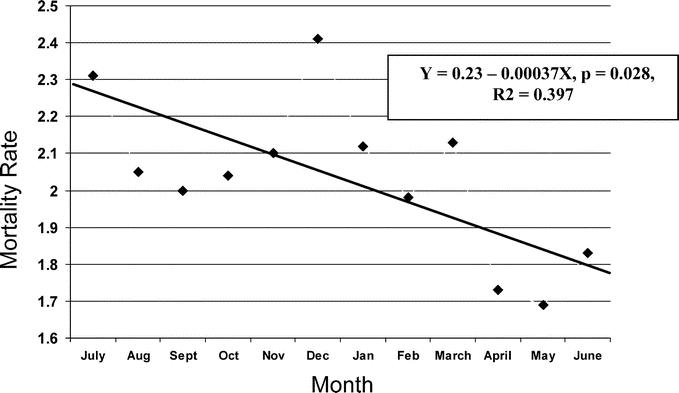
Results: There was 18% higher risk of postoperative morbidity in the early (n = 9941) versus the late group (n = 10313) (OR 1.18, 95%, CI 1.07-1.29, P = 0.0005, c-index 0.794). There was a 41% higher risk for mortality in the early group compared with the late group (OR 1.41, CI 1.11-1.80, P = 0.005, c-index 0.938). No significant trends in patient risk over time were noted.
Conclusion: Our data suggests higher rates of postsurgical morbidity and mortality related to the time of the year. Further study is needed to fully describe the etiologies of the seasonal variation in outcomes.
Figures
References
-
- Birkmeyer JD, Sun Y, Goldfaden A, et al. Volume and process of care in high-risk cancer surgery. Cancer. 2006;106:2476–2481. - PubMed
-
- Birkmeyer JD, Stukel TA, Siewers AE, et al. Surgeon volume and operative mortality in the United States. N Engl J Med. 2003;349:2117–2127. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–1137. - PubMed
-
- Helmreich RL, Merritt AC, Wilhlem JA. The evolution of crew resource management in training in commercial aviation. Int J Aviat Psychol. 1999;9:19–32. - PubMed
-
- Salas E, Burke CS, Bowers CA, et al. Team training in the skies: does crew resource management (CRM) training work? Hum Factors. 2001;43:641–674. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
