

A randomized multicenter trial to compare long-term functional outcome, quality of life, and complications of surgical procedures for low rectal cancers
- PMID: 17717452
- PMCID: PMC1959344
- DOI: 10.1097/SLA.0b013e3181485617
A randomized multicenter trial to compare long-term functional outcome, quality of life, and complications of surgical procedures for low rectal cancers
Abstract
Introduction: Colonic pouches have been used for 20 years to provide reservoir function after reconstructive proctectomy for rectal cancer. More recently coloplasty has been advocated as an alternative to a colonic pouch. However there have been no long-term randomized, controlled trials to compare functional outcomes of coloplasty, colonic J-Pouch (JP), or a straight anastomosis (SA) after the treatment of low rectal cancer.
Aim: : To compare the complications, long-term functional outcome, and quality of life (QOL) of patients undergoing a coloplasty, JP, or an SA in reconstruction of the lower gastrointestinal tract after proctectomy for low rectal cancer.
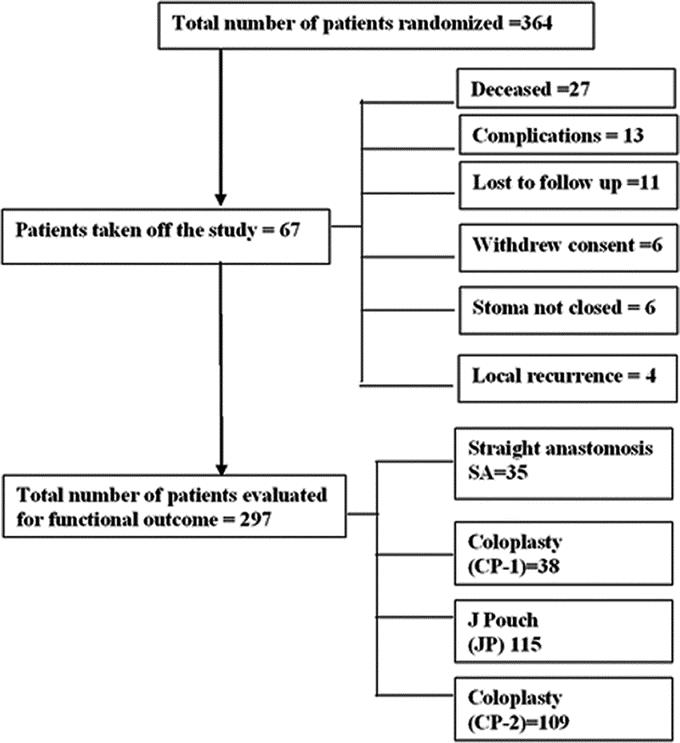
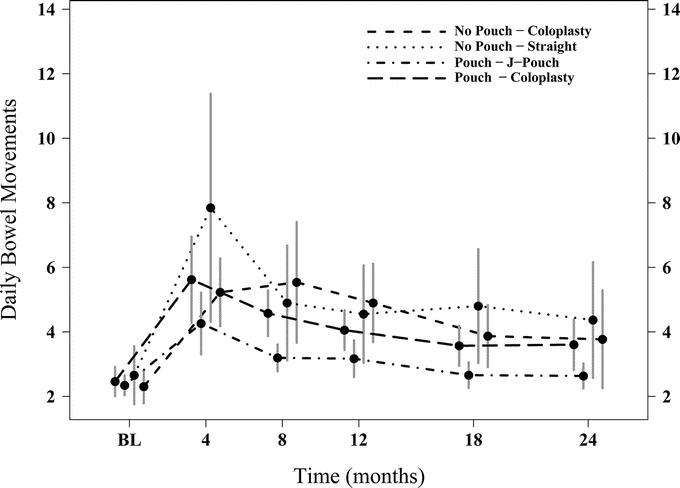
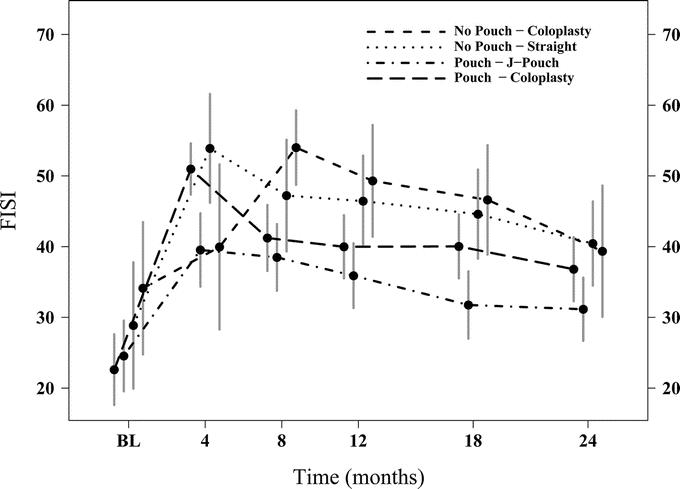
Methods: A multicenter study enrolled patients with low rectal cancer, who were randomized intraoperatively to coloplasty (CP-1) or SA if JP was not feasible, or JP or coloplasty (CP-2) if a JP was feasible. Patients were followed for 24 months with SF-36 surveys to evaluate the QOL. Bowel function was measured quantitatively and using Fecal Incontinence Severity Index (FISI). Urinary function and sexual function were also assessed.
Results: Three hundred sixty-four patients were randomized. All patients were evaluated for complications and recurrence. Mean age was 60 +/-12 years, 71% were male. Twenty-three (7.4%) died within 24 months of surgery. No significant difference was observed in the complications among the 4 groups. Two hundred ninety-seven of 364 were evaluated for functional outcome at 24 months. There was no difference in bowel function between the CP-1 and SA groups. JP patients had fewer bowel movements, less clustering, used fewer pads and had a lower FISI than the CP-2 group. Other parameters were not statistically different. QOL scores at 24 months were similar for each of the 4 groups.
Conclusions: In patients undergoing a restorative resection for low rectal cancer, a colonic JP offers significant advantages in function over an SA or a coloplasty. In patients who cannot have a pouch, coloplasty seems not to improve the bowel function of patients over that with an SA.
Figures
References
-
- Turnbull R Jr, Cuthbertson A. Abdominorectal pull-through resection for cancer and for Hirschsprung's disease. Delayed posterior colorectal anastomosis. Cleve Clin Q. 1961;28:109–115. - PubMed
-
- Goligher JC. Extended low anterior resection with stapled colorectal or coloanal anastomosis. Ann Chir Gynaecol. 1986;75:82–88. - PubMed
-
- Karanjia ND, Schache DJ, North WR, et al. Close shave in anterior resection. Br J Surg. 1990;77:510–512. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
