

Prognostic value of histopathology and trends in cervical cancer: a SEER population study
- PMID: 17718897
- PMCID: PMC1994954
- DOI: 10.1186/1471-2407-7-164
Prognostic value of histopathology and trends in cervical cancer: a SEER population study
Abstract
Background: Histopathology is a cornerstone in the diagnosis of cervical cancer but the prognostic value is controversial.
Methods: Women under active follow-up for histologically confirmed primary invasive cervical cancer were selected from the United States Surveillance, Epidemiology, and End Results (SEER) 9-registries public use data 1973-2002. Only histologies with at least 100 cases were retained. Registry area, age, marital status, race, year of diagnosis, tumor histology, grade, stage, tumor size, number of positive nodes, number of examined nodes, odds of nodal involvement, extent of surgery, and radiotherapy were evaluated in Cox models by stepwise selection using the Akaike Information Criteria.
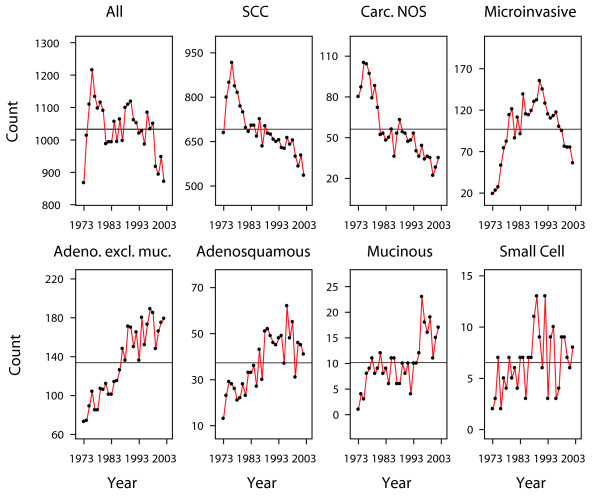
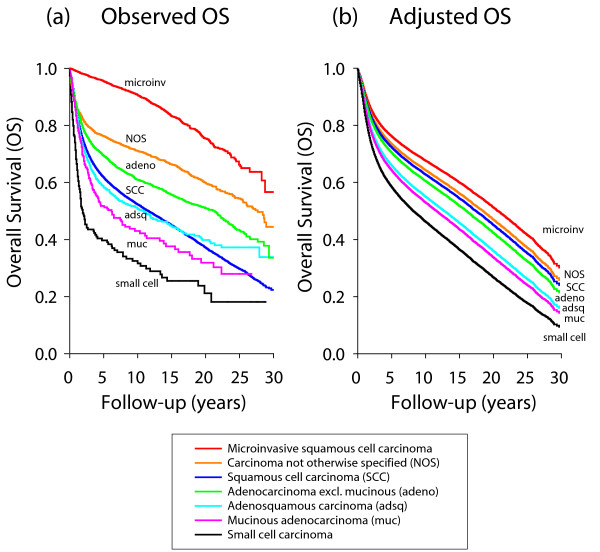
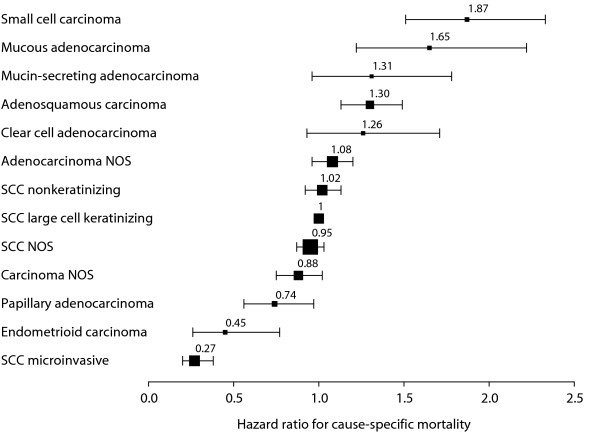
Results: There were 30,989 records evaluable. From 1973 to 2002, number of cases dropped from 1,100 new cases/year to 900/year, but adenocarcinomas and adenosquamous carcinoma increased from 100/year to 235/year. Median age was 48 years. Statistically significant variables for both overall and cause-specific mortality were: age, year of diagnosis, race, stage, histology, grade, hysterectomy, radiotherapy, tumor size and nodal ratio. The histological types were jointly significant, P < 0.001. Cause-specific mortality hazard ratios by histological type relatively to non-microinvasive squamous cell carcinoma were: microinvasive squamous cell carcinoma 0.28 (95% confidence interval: 0.20-0.39), carcinoma not otherwise specified 0.91 (0.79-1.04), non-mucinous adenocarcinoma 1.06 (0.98-1.15), adenosquamous carcinoma 1.35 (1.20-1.51), mucinous adenocarcinoma 1.52 (1.23-1.88), small cell carcinoma 1.94 (1.58-2.39).
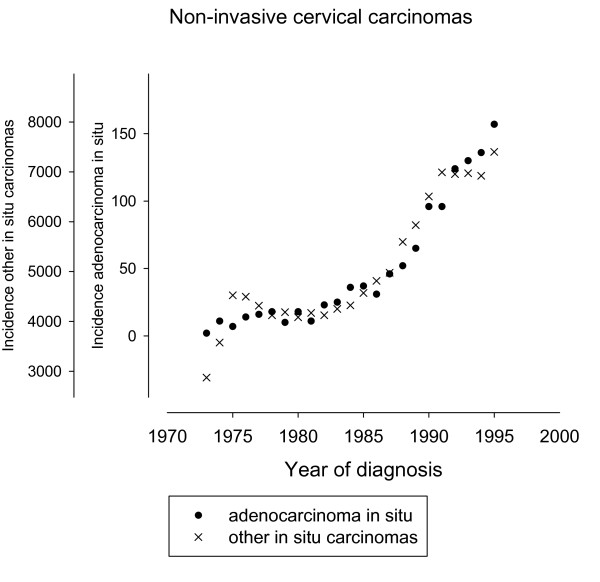
Conclusion: Small cell carcinoma and adenocarcinomas were associated with poorer survival. The incidental observation of increasing numbers of adenocarcinomas despite a general decline suggests the inefficiency of conventional screening for these tumors. Increased incidence of adenocarcinomas, their adverse prognosis, and the young age at diagnosis indicate the need to identify women who are at risk.
Figures
References
-
- Look KY, Brunetto VL, Clarke-Pearson DL, Averette HE, Major FJ, Alvarez RD, Homesley HD, Zaino RJ. An analysis of cell type in patients with surgically staged stage IB carcinoma of the cervix: a Gynecologic Oncology Group study. Gynecol Oncol. 1996;63:304–311. doi: 10.1006/gyno.1996.0327. - DOI - PubMed
