

Exploiting the apoptotic actions of oestrogen to reverse antihormonal drug resistance in oestrogen receptor positive breast cancer patients
- PMID: 17719781
- PMCID: PMC2707932
- DOI: 10.1016/j.breast.2007.07.020
Exploiting the apoptotic actions of oestrogen to reverse antihormonal drug resistance in oestrogen receptor positive breast cancer patients
Abstract
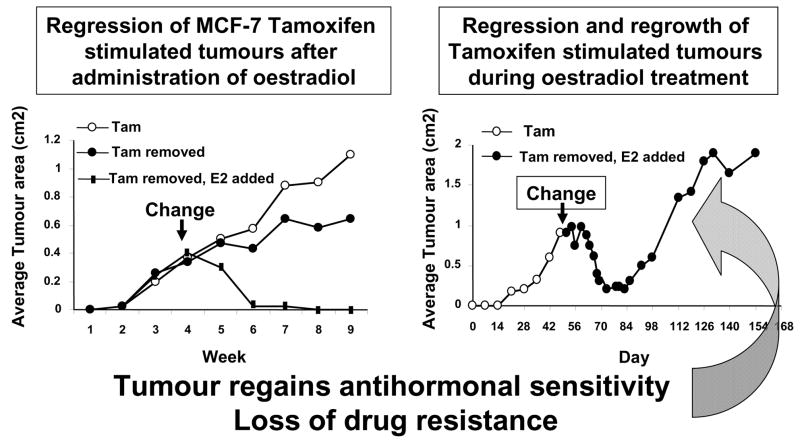
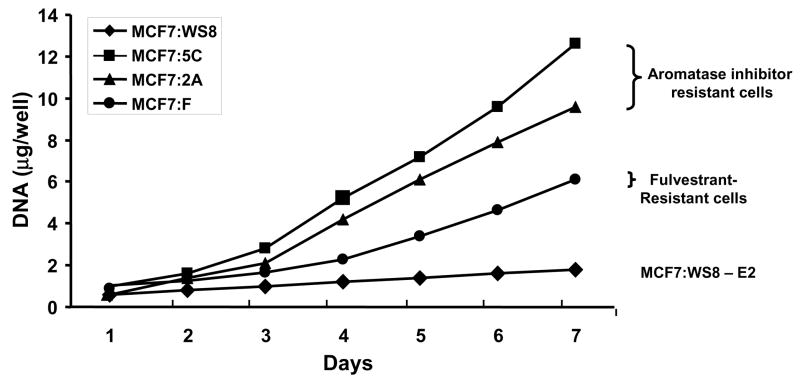
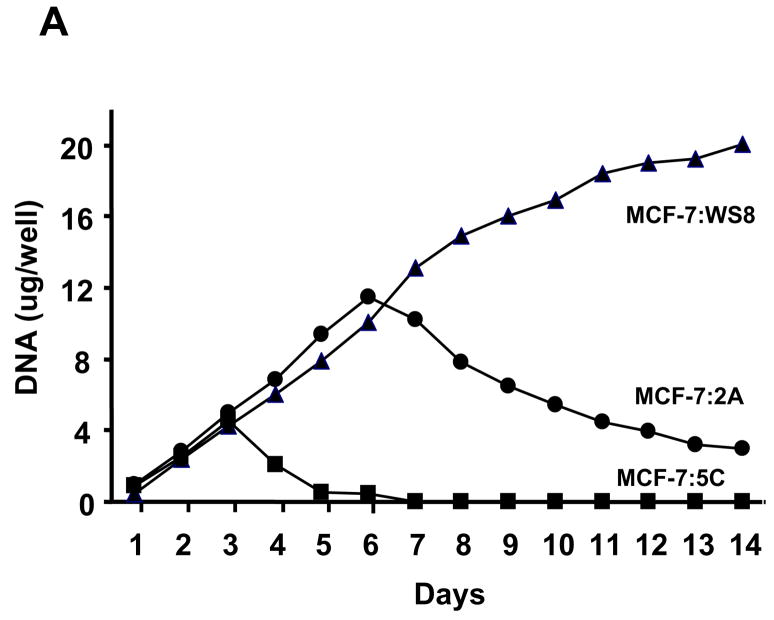
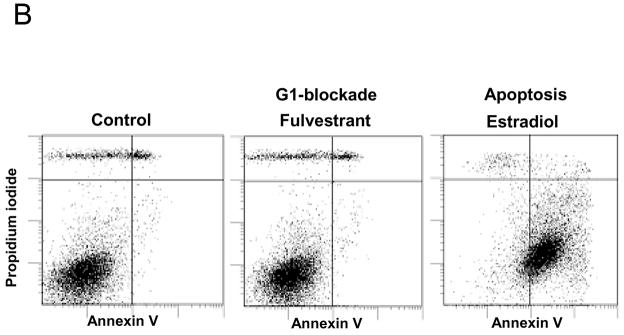
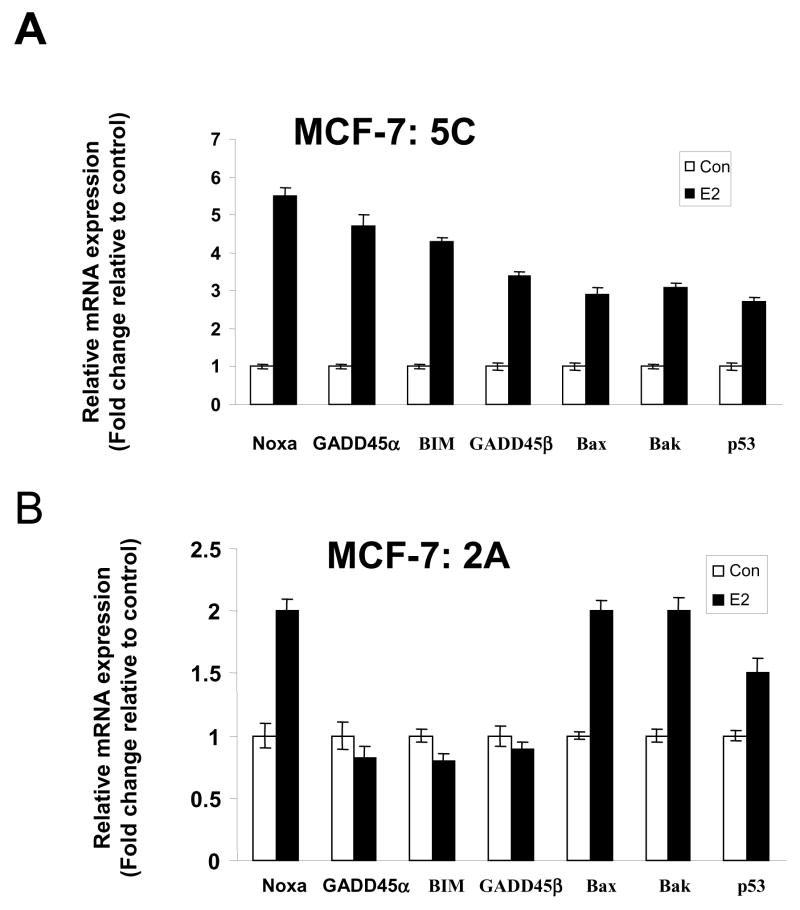
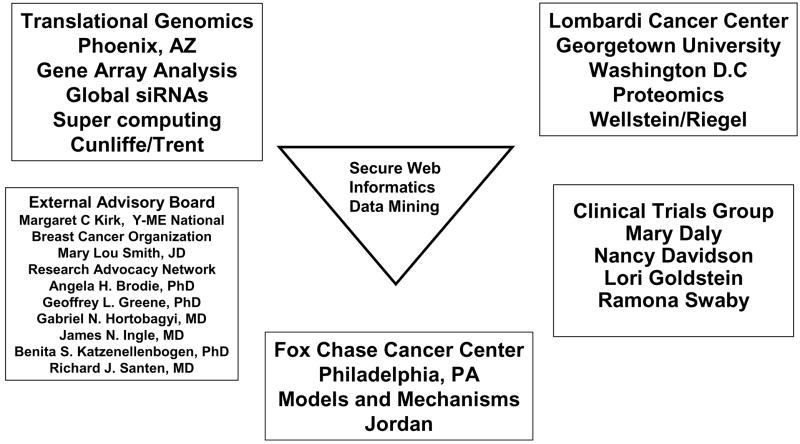
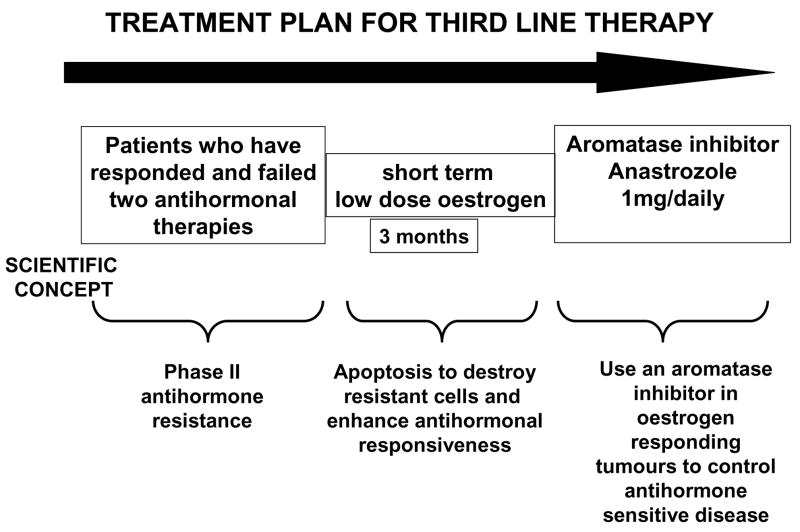
The ubiquitous application of selective oestrogen receptor modulators (SERMs) and aromatase inhibitors for the treatment and prevention of breast cancer has created a significant advance in patient care. However, the consequence of prolonged treatment with antihormonal therapy is the development of drug resistance. Nevertheless, the systematic description of models of drug resistance to SERMs and aromatase inhibitors has resulted in the discovery of a vulnerability in tumour homeostasis that can be exploited to improve patient care. Drug resistance to antihormones evolves, so that eventually the cells change to create novel signal transduction pathways for enhanced oestrogen (GPR30+OER) sensitivity, a reduction in progesterone receptor production and an increased metastatic potential. Most importantly, antihormone resistant breast cancer cells adapt with an ability to undergo apoptosis with low concentrations of oestrogen. The oestrogen destroys antihormone resistant cells and reactivates sensitivity to prolonged antihormonal therapy. We have initiated a major collaborative program of genomics and proteomics to use our laboratory models to map the mechanism of subcellular survival and apoptosis in breast cancer. The laboratory program is integrated with a clinical program that seeks to determine the minimum dose of oestrogen necessary to create objective responses in patients who have succeeded and failed two consecutive antihormonal therapies. Once our program is complete, the new knowledge will be available to translate to clinical care for the long-term maintenance of patients on antihormone therapy.
Figures
Similar articles
-
New hypotheses and opportunities in endocrine therapy: amplification of oestrogen-induced apoptosis.Breast. 2009 Oct;18 Suppl 3(Suppl 3):S10-7. doi: 10.1016/S0960-9776(09)70266-8. Breast. 2009. PMID: 19914527 Free PMC article.
-
Where do selective estrogen receptor modulators (SERMs) and aromatase inhibitors (AIs) now fit into breast cancer treatment algorithms?J Steroid Biochem Mol Biol. 2001 Dec;79(1-5):227-37. doi: 10.1016/s0960-0760(01)00140-6. J Steroid Biochem Mol Biol. 2001. PMID: 11850229 Review.
-
Estrogen-mediated mechanisms to control the growth and apoptosis of breast cancer cells: a translational research success story.Vitam Horm. 2013;93:1-49. doi: 10.1016/B978-0-12-416673-8.00007-1. Vitam Horm. 2013. PMID: 23810002 Review.
-
The apoptotic action of estrogen following exhaustive antihormonal therapy: a new clinical treatment strategy.Breast. 2005 Dec;14(6):624-30. doi: 10.1016/j.breast.2005.08.022. Epub 2005 Oct 3. Breast. 2005. PMID: 16202599 Review.
-
Low-dose estrogen therapy to reverse acquired antihormonal resistance in the treatment of breast cancer.Clin Breast Cancer. 2008 Apr;8(2):124-33. doi: 10.3816/CBC.2008.n.012. Clin Breast Cancer. 2008. PMID: 18621608 Review.
Cited by
-
Preclinical development of a neutral, estrogen receptor-targeted, tridentate 99mTc(I)-estradiol-pyridin-2-yl hydrazine derivative for imaging of breast and endometrial cancers.J Nucl Med. 2008 Jun;49(6):978-86. doi: 10.2967/jnumed.107.048546. Epub 2008 May 15. J Nucl Med. 2008. PMID: 18483091 Free PMC article.
-
New hypotheses and opportunities in endocrine therapy: amplification of oestrogen-induced apoptosis.Breast. 2009 Oct;18 Suppl 3(Suppl 3):S10-7. doi: 10.1016/S0960-9776(09)70266-8. Breast. 2009. PMID: 19914527 Free PMC article.
-
G protein-coupled estrogen receptor-selective ligands modulate endometrial tumor growth.Obstet Gynecol Int. 2013;2013:472720. doi: 10.1155/2013/472720. Epub 2013 Nov 27. Obstet Gynecol Int. 2013. PMID: 24379833 Free PMC article.
-
Signaling, physiological functions and clinical relevance of the G protein-coupled estrogen receptor GPER.Prostaglandins Other Lipid Mediat. 2009 Sep;89(3-4):89-97. doi: 10.1016/j.prostaglandins.2009.05.001. Epub 2009 May 13. Prostaglandins Other Lipid Mediat. 2009. PMID: 19442754 Free PMC article. Review.
-
Steroid hormone transforming aldo-keto reductases and cancer.Ann N Y Acad Sci. 2009 Feb;1155:33-42. doi: 10.1111/j.1749-6632.2009.03700.x. Ann N Y Acad Sci. 2009. PMID: 19250190 Free PMC article. Review.
References
-
- EBCTCG. Tamoxifen for early breast cancer: an overview of the randomised trials. Lancet. 1998;354:1451–67. - PubMed
-
- EBCTCG. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365:1687–717. - PubMed
-
- Howell A, Cuzick J, Baum M, et al. Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years’ adjuvant treatment for breast cancer. Lancet. 2005;365:60–62. - PubMed
-
- Thurlimann B, Keshaviah A, Coates AS, et al. A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med. 2005;353:2747–57. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
