

Congenital cavernous sinus cystic teratoma
- PMID: 17722246
- PMCID: PMC2628058
- DOI: 10.3349/ymj.2007.48.4.704
Congenital cavernous sinus cystic teratoma
Abstract
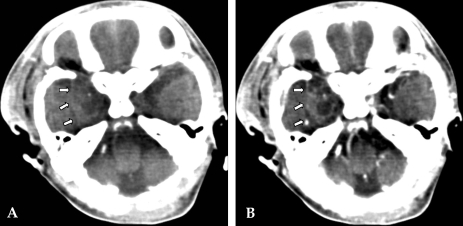
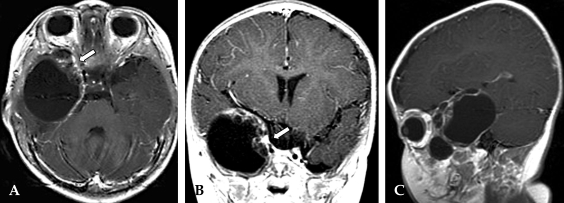
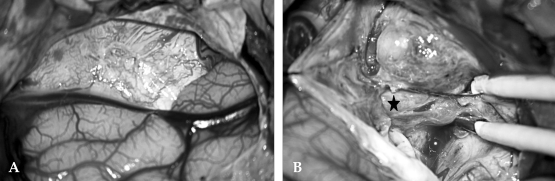
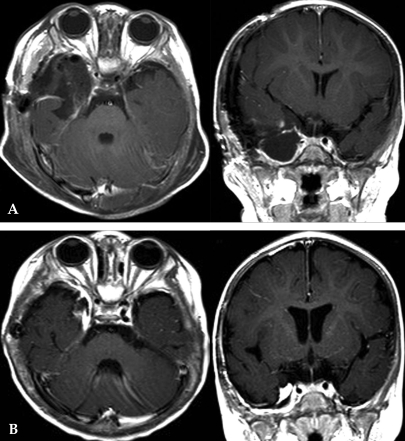
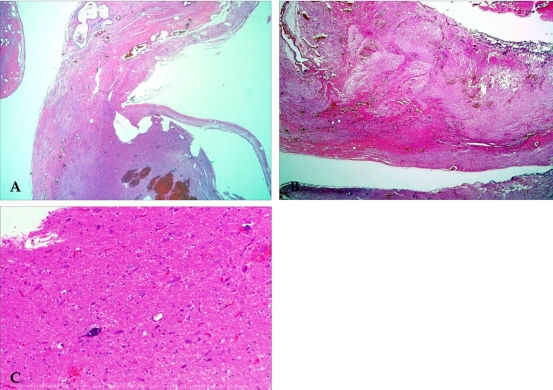
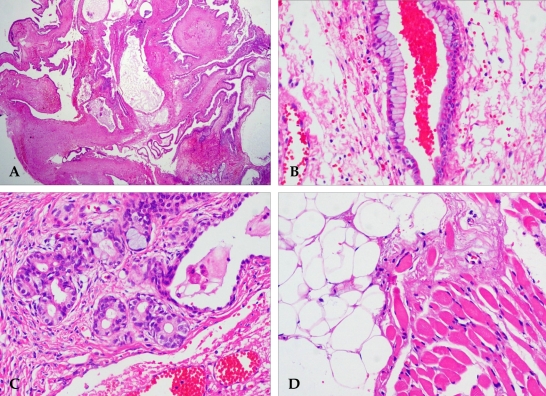
Teratomas represent 0.5% of all intracranial tumors. These benign tumors contain tissue representative of the three germinal layers. Most teratomas are midline tumors located predominantly in the sellar and pineal regions. The presence of a teratoma in the cavernous sinus is very rare. Congenital teratomas are also rare, especially those of a cystic nature. To our knowledge, this would be the first case report of a congenital, rapidly growing cystic teratoma within the cavernous sinus. A three-month-old boy presented with a past medical history of easy irritability and poor oral intake. A magnetic resonance image (MRI) scan of the head disclosed a large expanding cystic tumor filling the right cavernous sinus and extending into the pterygopalatine fossa through the foramen rotunda. These scans also demonstrated a small area of mixed signal intensity, the result of the different tissue types conforming to the tumor. Heterogeneous enhancement was seen after the infusion of contrast medium. However, this was a cystic tumor with a large cystic portion. Thus, a presumptive diagnosis of cystic glioma was made. With the use of a right frontotemporal approach, extradural dissection of the tumor was performed. The lesion entirely occupied the cavernous sinus, medially displacing the Gasserian ganglion and trigeminal branches (predominantly V1 and V2). The lesion was composed of different tissues, including fat, muscle and mature, brain-like tissue. The tumor was completely removed, and the pathological report confirmed the diagnosis of a mature teratoma. There was no evidence of recurrence. Despite the location of the lesion in the cavernous sinus, total removal can be achieved with the use of standard microsurgical techniques.
Figures
Similar articles
-
Giant cavernous sinus teratoma: a clinical example of a rare entity: case report.Neurosurgery. 2001 Jun;48(6):1367-70; discussion 1370-1. doi: 10.1097/00006123-200106000-00041. Neurosurgery. 2001. PMID: 11383744 Review.
-
Meningioma of the cavernous sinus in a child.Childs Nerv Syst. 1999 Jan;15(1):8-10. doi: 10.1007/s003810050318. Childs Nerv Syst. 1999. PMID: 10066014 Review.
-
Massive congenital intracranial immature teratoma of the lateral ventricle with retro-orbital extension: a case report and review of the literature.Pediatr Neurosurg. 2007;43(4):338-42. doi: 10.1159/000103319. Pediatr Neurosurg. 2007. PMID: 17627155 Review.
-
Giant interdural teratoma of the cavernous sinus.J Clin Neurosci. 2008 Dec;15(12):1414-6. doi: 10.1016/j.jocn.2007.04.028. Epub 2008 Oct 7. J Clin Neurosci. 2008. PMID: 18842410
-
Teratoma of the cavernous sinus: case report.Neurosurgery. 1995 May;36(5):1020-3. doi: 10.1227/00006123-199505000-00021. Neurosurgery. 1995. PMID: 7791967
References
-
- Becherer TA, Davis DG, Hodes JE, Warf BC. Intracavernous teratoma in a school-aged child. Pediatr Neurosurg. 1999;30:135–139. - PubMed
-
- Pikus HJ, Holmes B, Harbaugh RE. Teratoma of the cavernous sinus: case report. Neurosurgery. 1995;36:1020–1023. - PubMed
-
- Tobias S, Valarezo J, Meir K, Umansky F. Giant cavernous sinus teratoma: a clinical example of a rare entity: case report. Neurosurgery. 2001;48:1367–1371. - PubMed
-
- Shaffrey ME, Lanzino G, Lopes MB, Hessler RB, Kassell NF, VandenBerg SR. Maturation of intracranial immature teratomas. Report of two cases. J Neurosurg. 1996;85:672–676. - PubMed
-
- Hunt SJ, Johnson PC, Coons SW, Pittman HW. Neonatal intracranial teratomas. Surg Neurol. 1990;34:336–342. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
