

Usefulness of C-reactive protein in monitoring the severe community-acquired pneumonia clinical course
- PMID: 17723153
- PMCID: PMC2206486
- DOI: 10.1186/cc6105
Usefulness of C-reactive protein in monitoring the severe community-acquired pneumonia clinical course
Abstract
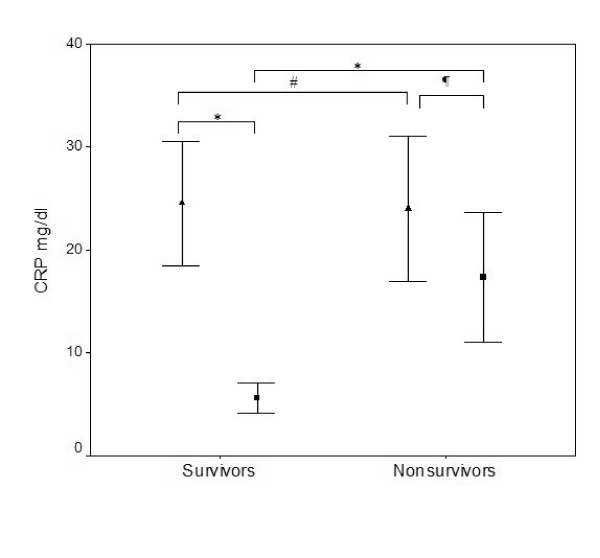
Background: The aim of the present study was to evaluate the C-reactive protein level, the body temperature and the white cell count in patients after prescription of antibiotics in order to describe the clinical resolution of severe community-acquired pneumonia.
Methods: A cohort of 53 consecutive patients with severe community-acquired pneumonia was studied. The C-reactive protein levels, body temperature and white cell count were monitored daily.
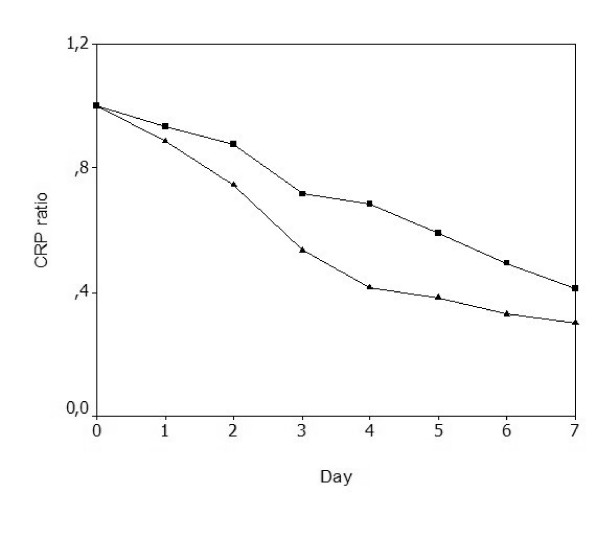
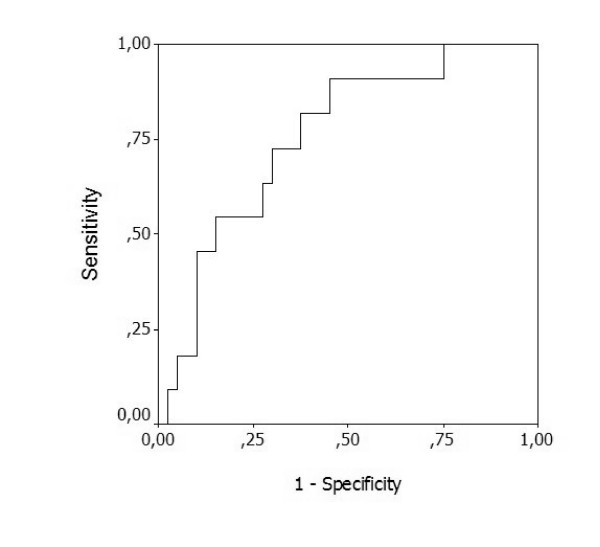
Results: By day 3 a C-reactive protein level 0.5 times the initial level was a marker of poor outcome (sensitivity, 0.91; specificity, 0.59). Patients were divided according to their C-reactive protein patterns of response to antibiotics, into fast response, slow response, nonresponse, and biphasic response. About 96% of patients with a C-reactive protein pattern of fast response and 74% of patients with a slow response pattern survived, whereas those patients with the patterns of nonresponse and of biphasic response had a mortality rate of 100% and 33%, respectively (P < 0.001). On day 3 of antibiotic therapy, a decrease in C-reactive protein levels by 0.31 or more from the previous day's level was a marker of good prognosis (sensitivity, 0.75; specificity, 0.85).
Conclusion: Daily C-reactive protein measurement after antibiotic prescription is useful in identification, as early as day 3, of severe community-acquired pneumonia patients with poor outcome. The identification of the C-reactive protein pattern of response to antibiotic therapy was useful in the recognition of the individual clinical course, either improving or worsening, as well as the rate of improvement, in patients with severe community-acquired pneumonia.
Figures
Comment in
-
A persistently elevated C-reactive protein level in pneumonia may indicate empyema.Crit Care. 2008;12(1):409; author reply 409. doi: 10.1186/cc6204. Crit Care. 2008. PMID: 18341702 Free PMC article. No abstract available.
References
-
- Niederman MS, Mandell LA, Anzueto A, Bass JB, Broughton WA, Campbell GD, Dean N, File T, Fine MJ, Gross PA, et al. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med. 2001;163:1730–1754. - PubMed
-
- Kaplan V, Angus DC, Griffin MF, Clermont G, Scott Watson R, Linde-Zwirble WT. Hospitalized community-acquired pneumonia in the elderly: age- and sex-related patterns of care and outcome in the United States. Am J Respir Crit Care Med. 2002;165:766–772. - PubMed
-
- Feinsilver SH, Fein AM, Niederman MS, Schultz DE, Faegenburg DH. Utility of fiberoptic bronchoscopy in nonresolving pneumonia. Chest. 1990;98:1322–1326. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
