

Intractable bleeding from solitary mandibular metastasis of hepatocellular carcinoma
- PMID: 17724815
- PMCID: PMC4611592
- DOI: 10.3748/wjg.v13.i33.4526
Intractable bleeding from solitary mandibular metastasis of hepatocellular carcinoma
Abstract
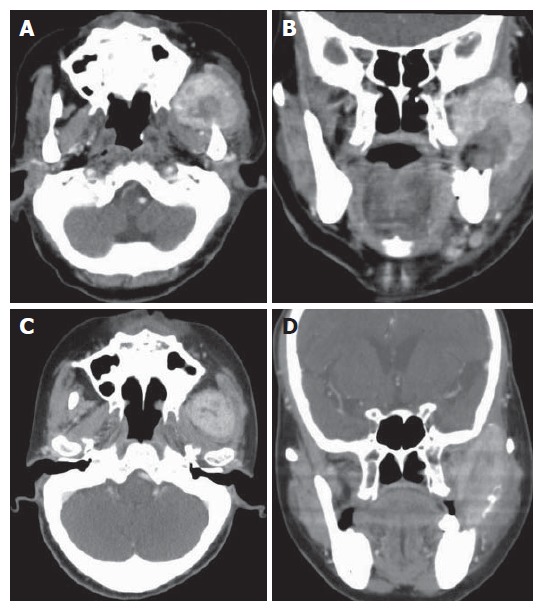
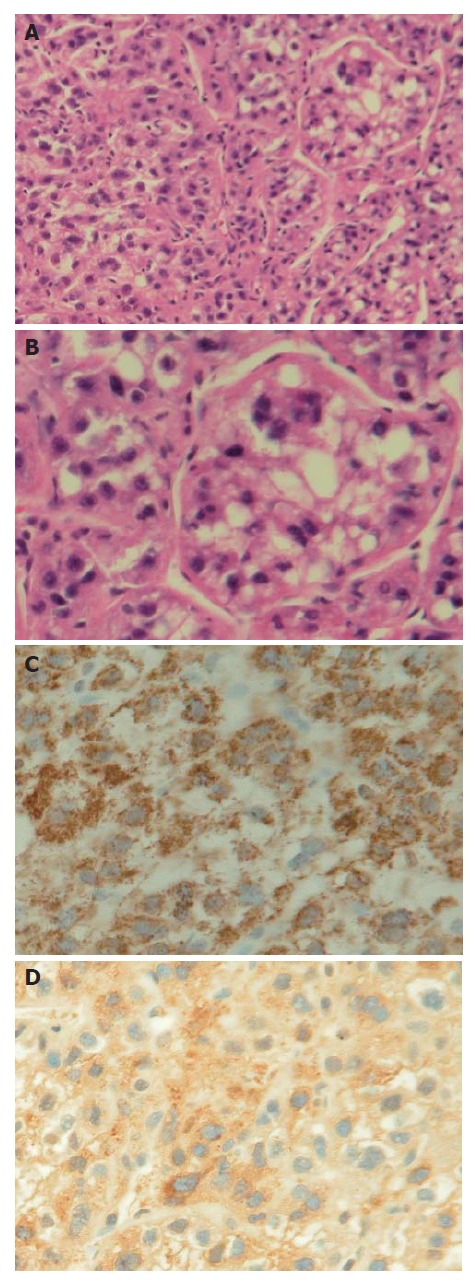
Hepatocellular carcinoma (HCC) metastasizes to the mandible is infrequently seen. Solitary bony metastasis to the mandible is rarer. The intractable bleeding caused by rupture of the metastatic HCC is challenging to clinicians. We present a case of a 74-year-old woman with HCC under control without progression for 3 years. Left facial swelling and episodes of bleeding developed recently and biopsy revealed a metastatic HCC. Computer tomography showed a large tumor in parapharyngeal space with evident mandibular ramus destruction. Bleeding occurred from the metastatic tumor but could not be controlled by electrocauterization, Surgical, tissue glue, and bone wax and angiographic embolization. Palliative radiotherapy (2400 cGy in 6 fractions) was tried and the intractable bleeding was successfully stopped after the radiotherapy. Because of the hypervascular and osteolytic nature of the solitary mandibular metastatic lesion, the bleeding was troublesome. Radiotherapy provided successful control of intractable bleeding from the metastatic tumor.
Figures
Similar articles
-
Mandibular metastatic hepatocellular carcinoma: report of a case involving severe and uncontrollable hemorrhage.Anticancer Res. 2001 May-Jun;21(3C):2121-30. Anticancer Res. 2001. PMID: 11501835
-
Mandibular metastatic hepatocellular carcinoma: a case involving severe postbiopsy hemorrhage.J Oral Maxillofac Surg. 1997 Jun;55(6):547-52. doi: 10.1016/s0278-2391(97)90480-8. J Oral Maxillofac Surg. 1997. PMID: 9191634 Review.
-
Solitary mandibular metastasis as an initial manifestation of hepatocellular carcinoma.Acta Med Okayama. 2006 Aug;60(4):243-7. doi: 10.18926/AMO/30713. Acta Med Okayama. 2006. PMID: 16943863
-
Hepatocellular carcinoma metastatic to the mandible.Ear Nose Throat J. 2013 Feb;92(2):E17-9. Ear Nose Throat J. 2013. PMID: 23460221
-
Hepatocellular carcinoma metastatic to the mandible: a case involving severe hemorrhage.Med Oral. 2004 Aug-Oct;9(4):345-9. Med Oral. 2004. PMID: 15292875 Review. English, Spanish.
Cited by
-
Two rare forms of hepatocellular carcinoma metastases.BMJ Case Rep. 2013 Jun 10;2013:bcr2013008886. doi: 10.1136/bcr-2013-008886. BMJ Case Rep. 2013. PMID: 23761493 Free PMC article.
-
Metastasis to the Jawbones: A review of 453 cases.J Int Soc Prev Community Dent. 2017 Mar-Apr;7(2):71-81. doi: 10.4103/jispcd.JISPCD_512_16. Epub 2017 Mar 29. J Int Soc Prev Community Dent. 2017. PMID: 28462174 Free PMC article. Review.
-
Scapular metastasis of hepatocellular carcinoma presenting as acute bleeding and hematoma: A case report of safe and effective treatment.Medicine (Baltimore). 2017 Nov;96(46):e8736. doi: 10.1097/MD.0000000000008736. Medicine (Baltimore). 2017. PMID: 29145320 Free PMC article.
-
Metastasis to the oral soft tissues: A review of 412 cases.J Int Soc Prev Community Dent. 2016 Sep-Oct;6(5):393-401. doi: 10.4103/2231-0762.192935. Epub 2016 Oct 24. J Int Soc Prev Community Dent. 2016. PMID: 27891304 Free PMC article. Review.
-
A collision tumor composed of colon adenocarcinoma and large cell neuroendocrine carcinoma with gingival metastasis: a case report.Front Oncol. 2025 Aug 6;15:1633770. doi: 10.3389/fonc.2025.1633770. eCollection 2025. Front Oncol. 2025. PMID: 40842588 Free PMC article.
References
-
- Kao JH, Chen DS. Changing disease burden of hepatocellular carcinoma in the Far East and Southeast Asia. Liver Int. 2005;25:696–703. - PubMed
-
- Yoshimura Y, Matsuda S, Naitoh S. Hepatocellular carcinoma metastatic to the mandibular ramus and condyle: report of a case and review of the literature. J Oral Maxillofac Surg. 1997;55:297–306. - PubMed
-
- Lee YT, Geer DA. Primary liver cancer: pattern of metastasis. J Surg Oncol. 1987;36:26–31. - PubMed
-
- Fukutomi M, Yokota M, Chuman H, Harada H, Zaitsu Y, Funakoshi A, Wakasugi H, Iguchi H. Increased incidence of bone metastases in hepatocellular carcinoma. Eur J Gastroenterol Hepatol. 2001;13:1083–1088. - PubMed
-
- Batson OV. The function of the vertebral veins and their role in the spread of metastases. 1940. Clin Orthop Relat Res. 1995:4–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
