

Mucin-hypersecreting bile duct neoplasm characterized by clinicopathological resemblance to intraductal papillary mucinous neoplasm (IPMN) of the pancreas
- PMID: 17725824
- PMCID: PMC2000466
- DOI: 10.1186/1477-7819-5-98
Mucin-hypersecreting bile duct neoplasm characterized by clinicopathological resemblance to intraductal papillary mucinous neoplasm (IPMN) of the pancreas
Abstract
Background: Although intraductal papillary mucinous neoplasm (IPMN) of the pancreas is acceptable as a distinct disease entity, the concept of mucin-secreting biliary tumors has not been fully established.
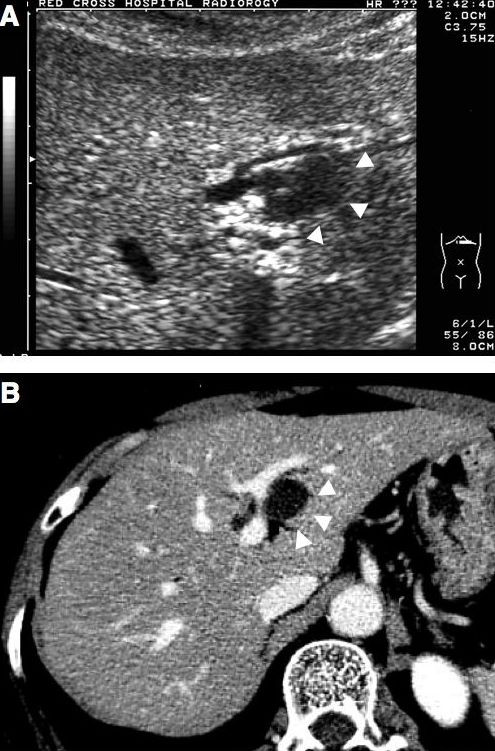
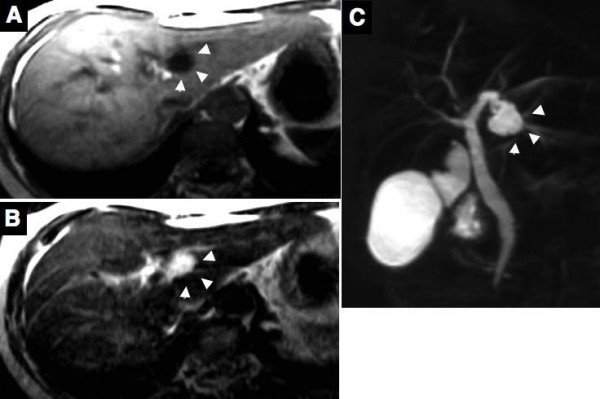
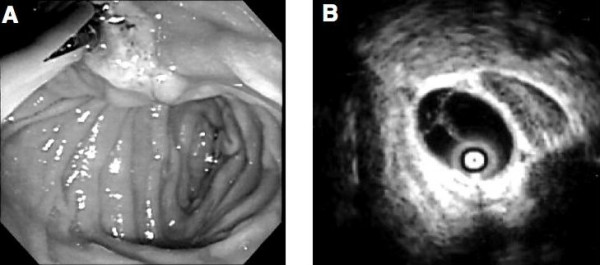
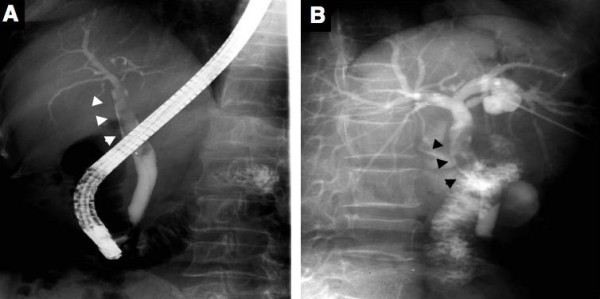
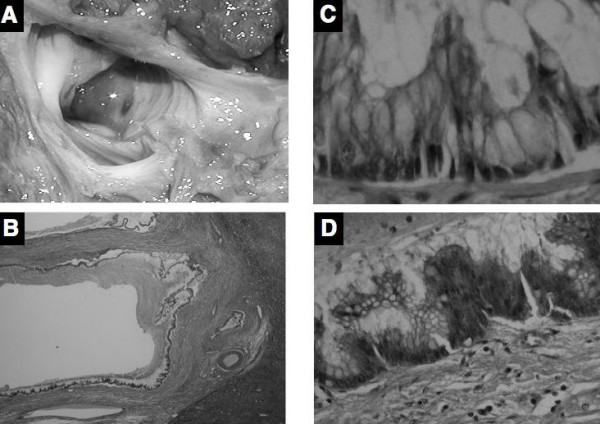
Case presentation: We describe herein a case of mucin secreting biliary neoplasm. Imaging revealed a cystic lesion 2 cm in diameter at the left lateral segment of the liver. Duodenal endoscopy revealed mucin secretion through an enlarged papilla of Vater. On the cholangiogram, the cystic lesion communicated with bile duct, and large filling defects caused by mucin were observed in the dilated common bile duct. This lesion was diagnosed as a mucin-secreting bile duct tumor. Left and caudate lobectomy of the liver with extrahepatic bile duct resection and reconstruction was performed according to the possibility of the tumor's malignant behavior. Histological examination of the specimen revealed biliary cystic wall was covered by micropapillary neoplastic epithelium with mucin secretion lacking stromal invasion nor ovarian-like stroma. The patient has remained well with no evidence of recurrence for 38 months since her operation.
Conclusion: It is only recently that the term "intraductal papillary mucinous neoplasm (IPMN)," which is accepted as a distinct disease entity of the pancreas, has begun to be used for mucin-secreting bile duct tumor. This case also seemed to be intraductal papillary neoplasm with prominent cystic dilatation of the bile duct.
Figures
Similar articles
-
Mucin-secreting bile duct adenoma--clinicopathological resemblance to intraductal papillary mucinous tumor of the pancreas.Dig Surg. 2002;19(4):324-7. doi: 10.1159/000064570. Dig Surg. 2002. PMID: 12207078
-
Cyst-forming intraductal papillary neoplasm of the bile ducts: description of imaging and pathologic aspects.AJR Am J Roentgenol. 2011 Nov;197(5):1111-20. doi: 10.2214/AJR.10.6363. AJR Am J Roentgenol. 2011. PMID: 22021503
-
Immunohistochemical characteristics and malignant progression of hepatic cystic neoplasms in comparison with pancreatic counterparts.Hum Pathol. 2012 Dec;43(12):2177-86. doi: 10.1016/j.humpath.2012.03.007. Epub 2012 Jun 15. Hum Pathol. 2012. PMID: 22705005
-
Intraductal papillary mucininous neoplasm of the bile ducts: multimodality assessment with pathologic correlation.Abdom Imaging. 2011 Aug;36(4):447-56. doi: 10.1007/s00261-010-9649-x. Abdom Imaging. 2011. PMID: 20959978 Review.
-
Mucinous Cystic Neoplasm of the Liver or Intraductal Papillary Mucinous Neoplasm of the Bile Duct? A Case Report and a Review of Literature.Ann Hepatol. 2018 May-June;17(3):519-524. doi: 10.5604/01.3001.0011.7397. Epub 2018 Apr 9. Ann Hepatol. 2018. PMID: 29735801 Review.
Cited by
-
Gallbladder Papillary Neoplasia Associated With Intrahepatic Carcinoma and Pancreaticobiliary Malformation.Gastroenterology Res. 2012 Dec;5(6):245-248. doi: 10.4021/gr505e. Epub 2012 Nov 20. Gastroenterology Res. 2012. PMID: 27785217 Free PMC article.
-
Intraductal papillary mucinous tumor of bile ducts radiologic and pathologic features: a case report.Cases J. 2008 Nov 17;1(1):319. doi: 10.1186/1757-1626-1-319. Cases J. 2008. PMID: 19014697 Free PMC article.
-
Gd-EOB-DTPA-enhanced magnetic resonance imaging for bile duct intraductal papillary mucinous neoplasms.World J Gastroenterol. 2015 Jul 7;21(25):7824-33. doi: 10.3748/wjg.v21.i25.7824. World J Gastroenterol. 2015. PMID: 26167082 Free PMC article.
-
Biliary tract intraductal papillary mucinous neoplasm: report of 19 cases.World J Gastroenterol. 2015 Apr 14;21(14):4261-7. doi: 10.3748/wjg.v21.i14.4261. World J Gastroenterol. 2015. PMID: 25892877 Free PMC article.
-
Intraductal papillary mucinous neoplasm of the biliary tract: a real disease?HPB (Oxford). 2009 Dec;11(8):684-91. doi: 10.1111/j.1477-2574.2009.00122.x. HPB (Oxford). 2009. PMID: 20495637 Free PMC article.
References
-
- Sakamoto E, Hayakawa N, Kamiya J, Kondo S, Nagino M, Kanai M, Miyachi M, Uesaka K, Nimura Y. Treatment strategy for mucin-producing intrahepatic cholangiocarcinoma: Value of percutaneous transhepatic biliary drainage and cholangioscopy. World J Surg. 1999;23:1038–1044. doi: 10.1007/s002689900620. - DOI - PubMed
-
- Styne P, Warren GH, Kumpe DA, Halgrimson C, Kern F., Jr Obstructive cholangitis secondary to mucus secreted by a solitary papillary bile duct tumor. Gastroenterology. 1986;90:748–753. - PubMed
-
- Wang YL, Lee SD, Lai KH, Wang SS, Lo KJ. Primary biliary cystic tumors of the liver. Am J Gastroenterol. 1993;88:599–603. - PubMed
-
- Longnecker DS, Hruban RH, Adler G, Kloppel G. Intraductal papillary-mucinous neoplasm of the pancreas; World Health Organization International Histological Classification of Tumors, Pathology and Genetics of Tumours of the Digestive System. Lyon, France: IARC Press; 2000. pp. 237–240.
LinkOut - more resources
Full Text Sources
