

Duloxetine in the treatment of major depressive disorder: an open-label study
- PMID: 17725843
- PMCID: PMC2018694
- DOI: 10.1186/1471-244X-7-43
Duloxetine in the treatment of major depressive disorder: an open-label study
Abstract
Background: Major depressive disorder (MDD) is a chronic and highly disabling condition. Existing pharmacotherapies produce full remission in only 30% to 40% of treated patients. Antidepressants exhibiting dual reuptake inhibition of both serotonin (5-HT) and norepinephrine (NE) may achieve higher rates of remission compared with those acting upon a single neurotransmitter. In this study, the safety and efficacy of duloxetine, a potent dual reuptake inhibitor of 5-HT and NE, were examined.
Methods: Patients (N = 533) meeting DSM-IV criteria for MDD received open-label duloxetine (60 mg once a day [QD]) for 12 weeks during the initial phase of a relapse prevention trial. Patients were required to have a 17-item Hamilton Rating Scale for Depression (HAMD17) total score >or=18 and a Clinical Global Impression of Severity (CGI-S) score >or=4 at baseline. Efficacy measures included the HAMD17 total score, HAMD17 subscales, the CGI-S, the Patient Global Impression of Improvement (PGI-I) scale, Visual Analog Scales (VAS) for pain, and the Symptom Questionnaire, Somatic Subscale (SQ-SS). Quality of life was assessed using the Sheehan Disability Scale (SDS) and the Quality of Life in Depression Scale (QLDS). Safety was evaluated by recording spontaneously-reported treatment-emergent adverse events, changes in vital signs and laboratory analytes, and the Patient Global Impression of Sexual Function (PGI-SF) scale.
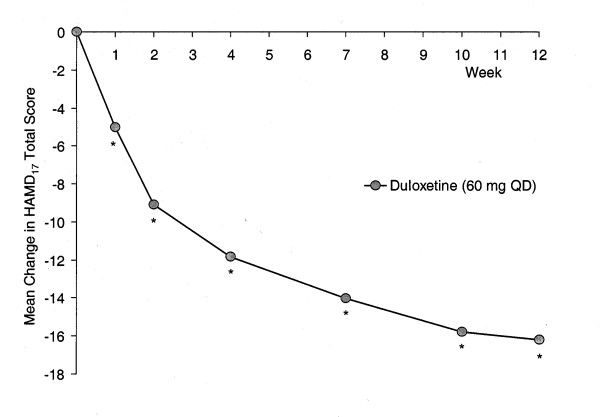
Results: The rate of discontinuation due to adverse events was 11.3%. Treatment-emergent adverse events reported by >or=10% duloxetine-treated patients were nausea, headache, dry mouth, somnolence, insomnia, and dizziness. Following 12 weeks of open-label duloxetine therapy, significant improvements were observed in all assessed efficacy and quality of life measures. In assessments of depression severity (HAMD17, CGI-S) the magnitude of symptom improvement continued to increase at each study visit, while for painful physical symptoms the onset of improvement was rapid and reached a maximum after 2 to 3 weeks of treatment.
Conclusion: In this open-label phase of a relapse prevention study, duloxetine (60 mg QD) was shown to be safe and effective in the treatment of MDD.
Trial registration: ClinicalTrials.gov NCT00036309.
Figures

Similar articles
-
Duloxetine 60 mg once-daily in the treatment of painful physical symptoms in patients with major depressive disorder.J Psychiatr Res. 2005 Jan;39(1):43-53. doi: 10.1016/j.jpsychires.2004.04.011. J Psychiatr Res. 2005. PMID: 15504423 Clinical Trial.
-
Duloxetine for the treatment of major depressive disorder: a closer look at efficacy and safety data across the approved dose range.J Psychiatr Res. 2006 Jun;40(4):337-48. doi: 10.1016/j.jpsychires.2005.08.010. Epub 2005 Nov 4. J Psychiatr Res. 2006. PMID: 16271726
-
Duloxetine in the acute and long-term treatment of major depressive disorder: a placebo- and paroxetine-controlled trial.Eur Neuropsychopharmacol. 2004 Dec;14(6):457-70. doi: 10.1016/j.euroneuro.2004.01.002. Eur Neuropsychopharmacol. 2004. PMID: 15589385 Clinical Trial.
-
Duloxetine: a review of its use in the treatment of generalized anxiety disorder.CNS Drugs. 2009;23(6):523-41. doi: 10.2165/00023210-200923060-00006. CNS Drugs. 2009. PMID: 19480470 Review.
-
Patterns of depressive symptom response in duloxetine-treated outpatients with mild, moderate or more severe depression.Int J Clin Pract. 2007 Aug;61(8):1337-48. doi: 10.1111/j.1742-1241.2007.01444.x. Int J Clin Pract. 2007. PMID: 17627710 Review.
Cited by
-
Antidepressant medication treatment patterns in Asian patients with major depressive disorder.Patient Prefer Adherence. 2015 Mar 11;9:421-8. doi: 10.2147/PPA.S68432. eCollection 2015. Patient Prefer Adherence. 2015. PMID: 25792815 Free PMC article.
-
Functional improvement and correlations with symptomatic improvement in adults with attention deficit hyperactivity disorder receiving long-acting methylphenidate.Psychol Med. 2012 Jan;42(1):195-204. doi: 10.1017/S0033291711000845. Epub 2011 Jun 1. Psychol Med. 2012. PMID: 21733214 Free PMC article. Clinical Trial.
-
Study of Sex Differences in Duloxetine Efficacy for Depression in Transgenic Mouse Models.Front Cell Neurosci. 2017 Oct 31;11:344. doi: 10.3389/fncel.2017.00344. eCollection 2017. Front Cell Neurosci. 2017. PMID: 29163055 Free PMC article.
-
Disability and treatment of specific mental and physical disorders across the world.Br J Psychiatry. 2008 May;192(5):368-75. doi: 10.1192/bjp.bp.107.039107. Br J Psychiatry. 2008. PMID: 18450663 Free PMC article.
-
Prevalence of dry eye disease among US men: estimates from the Physicians' Health Studies.Arch Ophthalmol. 2009 Jun;127(6):763-8. doi: 10.1001/archophthalmol.2009.103. Arch Ophthalmol. 2009. PMID: 19506195 Free PMC article. Clinical Trial.
References
-
- Greden JF. The burden of recurrent depression: causes, consequences, and future prospects. J Clin Psychiatry. 2001;62:5–9. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
