

Accuracy of electrocardiography in diagnosis of left ventricular hypertrophy in arterial hypertension: systematic review
- PMID: 17726091
- PMCID: PMC2001078
- DOI: 10.1136/bmj.39276.636354.AE
Accuracy of electrocardiography in diagnosis of left ventricular hypertrophy in arterial hypertension: systematic review
Abstract
Objective: To review the accuracy of electrocardiography in screening for left ventricular hypertrophy in patients with hypertension.
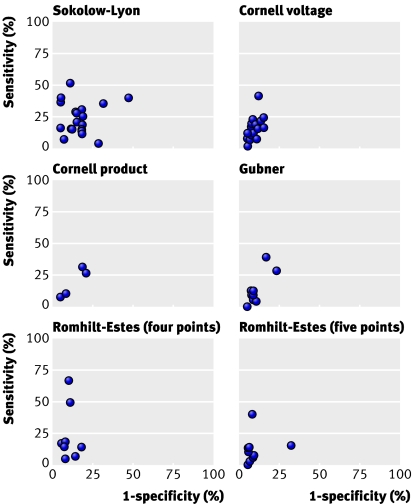
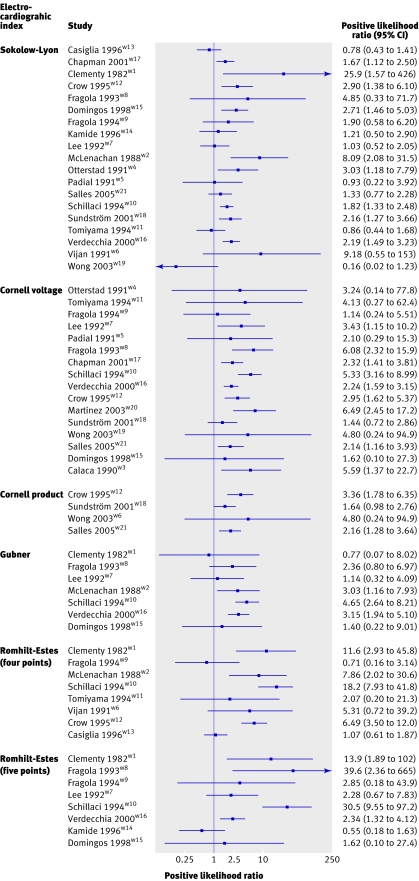
Design: Systematic review of studies of test accuracy of six electrocardiographic indexes: the Sokolow-Lyon index, Cornell voltage index, Cornell product index, Gubner index, and Romhilt-Estes scores with thresholds for a positive test of > or =4 points or > or =5 points.
Data sources: Electronic databases ((Pre-)Medline, Embase), reference lists of relevant studies and previous reviews, and experts.
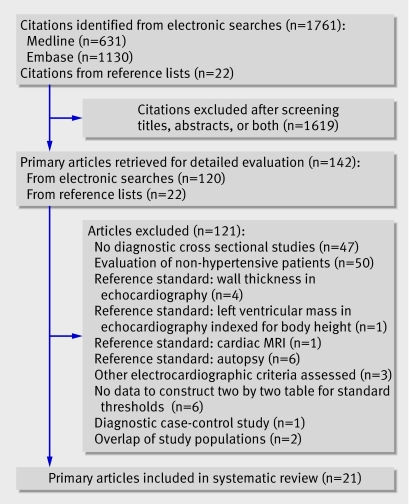
Study selection: Two reviewers scrutinised abstracts and examined potentially eligible studies. Studies comparing the electrocardiographic index with echocardiography in hypertensive patients and reporting sufficient data were included.
Data extraction: Data on study populations, echocardiographic criteria, and methodological quality of studies were extracted.
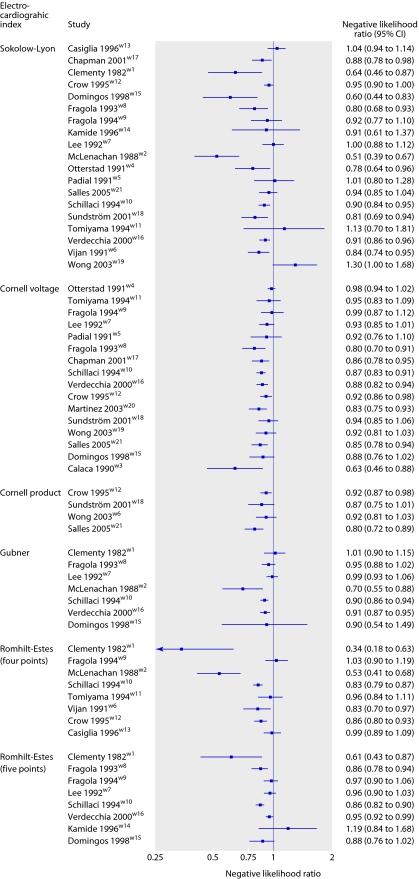
Data synthesis: Negative likelihood ratios, which indicate to what extent the posterior odds of left ventricular hypertrophy is reduced by a negative test, were calculated.
Results: 21 studies and data on 5608 patients were analysed. The median prevalence of left ventricular hypertrophy was 33% (interquartile range 23-41%) in primary care settings (10 studies) and 65% (37-81%) in secondary care settings (11 studies). The median negative likelihood ratio was similar across electrocardiographic indexes, ranging from 0.85 (range 0.34-1.03) for the Romhilt-Estes score (with threshold > or =4 points) to 0.91 (0.70-1.01) for the Gubner index. Using the Romhilt-Estes score in primary care, a negative electrocardiogram result would reduce the typical pre-test probability from 33% to 31%. In secondary care the typical pre-test probability of 65% would be reduced to 63%.
Conclusion: Electrocardiographic criteria should not be used to rule out left ventricular hypertrophy in patients with hypertension.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Diagnosing left ventricular hypertrophy in arterial hypertension.BMJ. 2007 Oct 6;335(7622):681-2. doi: 10.1136/bmj.39344.470718.BE. BMJ. 2007. PMID: 17916817 Free PMC article.
-
Ethnicity is relevant.BMJ. 2007 Oct 20;335(7624):787. doi: 10.1136/bmj.39367.371736.BE. BMJ. 2007. PMID: 17947749 Free PMC article. No abstract available.
-
QRS voltage criteria can be useful.BMJ. 2007 Oct 20;335(7624):787. doi: 10.1136/bmj.39367.394155.BE. BMJ. 2007. PMID: 17947750 Free PMC article. No abstract available.
-
A scientifically based technique.Dtsch Arztebl Int. 2008 Apr;105(15):292; author reply 292. doi: 10.3238/arztebl.2008.0292a. Epub 2008 Apr 11. Dtsch Arztebl Int. 2008. PMID: 19629235 Free PMC article. No abstract available.
References
-
- Kannel WB, Gordon T, Offutt D. Left ventricular hypertrophy by electrocardiogram: prevalence, incidence, and mortality in the Framingham study. Ann Intern Med 1969;71:89-105. - PubMed
-
- Kannel WB, Gordon T, Castelli WP, Margolis JR. Electrocardiographic left ventricular hypertrophy and risk of coronary heart disease: the Framingham study. Ann Intern Med 1970;72:813-22. - PubMed
-
- Haider AW, Larson MG, Benjamin EJ, Levy D. Increased left ventricular mass and hypertrophy are associated with increased risk for sudden death. J Am Coll Cardiol 1998;32:1454-9. - PubMed
-
- Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Gattobigio R, Zampi I, et al. Prognostic value of a new electrocardiographic method for diagnosis of left ventricular hypertrophy in essential hypertension. J Am Coll Cardiol 1998;31:383-90. - PubMed
-
- Sundström J, Lind L, Arnlöv J, Zethelius B, Andrén B, Lithell HO. Echocardiographic and electrocardiographic diagnoses of left ventricular hypertrophy predict mortality independently of each other in a population of elderly men. Circulation 2001;103:2346-51. - PubMed