

Excess mortality following hip fracture: the role of underlying health status
- PMID: 17726622
- PMCID: PMC2729704
- DOI: 10.1007/s00198-007-0429-6
Excess mortality following hip fracture: the role of underlying health status
Abstract
We evaluated the long-term excess mortality associated with hip fracture, using prospectively collected data on pre-fracture health and function from a nationally representative sample of U.S. elders. Although mortality was elevated for the first six months following hip fracture, we found no evidence of long-term excess mortality.
Introduction: The long-term excess mortality associated with hip fracture remains controversial.
Methods: To assess the association between hip fracture and mortality, we used prospectively collected data on pre-fracture health and function from a representative sample of U.S. elders in the Medicare Current Beneficiary Survey (MCBS) to perform survival analyses with time-varying covariates.
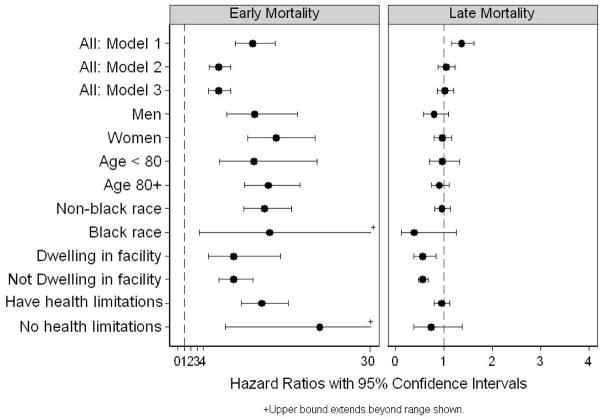
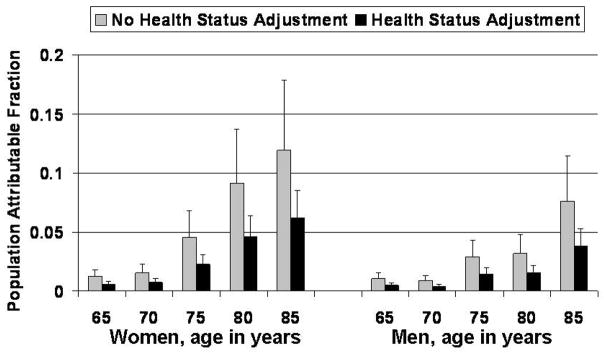
Results: Among 25,178 MCBS participants followed for a median duration of 3.8 years, 730 sustained a hip fracture during follow-up. Both early (within 6 months) and subsequent mortality showed significant elevations in models adjusted only for age, sex and race. With additional adjustment for pre-fracture health status, functional impairments, comorbid conditions and socioeconomic status, however, increased mortality was limited to the first six months after fracture (hazard ratio [HR]: 6.28, 95% CI: 4.82, 8.19). No increased mortality was evident during subsequent follow-up (HR: 1.04, 95% CI: 0.88, 1.23). Hip-fracture-attributable population mortality ranged from 0.5% at age 65 among men to 6% at age 85 among women.
Conclusions: Hip fracture was associated with substantially increased mortality, but much of the short-term risk and all of the long-term risk was explained by the greater frailty of those experiencing hip fracture.
Figures
References
-
- Melton LJ., III Adverse outcomes of osteoporotic fractures in the general population. J Bone Miner Res. 2003;18:1139–1141. - PubMed
-
- Vanness D, Tosteson A. Estimating the opportunity costs of osteoporosis in the United States. Topics Geriatric Rehab. 2005;21:4–16.
-
- Office of the Surgeon General. Bone Health and Osteoporosis: A report of the Surgeon General. U.S. Department of Health and Human Services; Rockville, MD: 2004. - PubMed
-
- Kanis JA, Borgstrom F, Zethraeus N, Johnell O, Oden A, Jonsson B. Intervention thresholds for osteoporosis in the UK. Bone. 2005;36:22–32. - PubMed
-
- Kanis JA, Johnell O, Oden A, Borgstrom F, Johansson H, De Laet C, Jonsson B. Intervention thresholds for osteoporosis in men and women: a study based on data from Sweden. Osteoporos Int. 2005;16:6–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
