

Signs and symptoms for diagnosis of serious infections in children: a prospective study in primary care
- PMID: 17727746
- PMCID: PMC2099636
Signs and symptoms for diagnosis of serious infections in children: a prospective study in primary care
Abstract
Background: Serious infections in children (sepsis, meningitis, pneumonia, pyelonephritis, osteomyelitis, and cellulitis) are associated with considerable mortality and morbidity. In children with an acute illness, the primary care physician uses signs and symptoms to assess the probability of a serious infection and decide on further management.
Aim: To analyse the diagnostic accuracy of signs and symptoms, and to create a multivariable triage instrument.
Design of study: A prospective diagnostic accuracy study.
Setting: Primary care in Belgium.
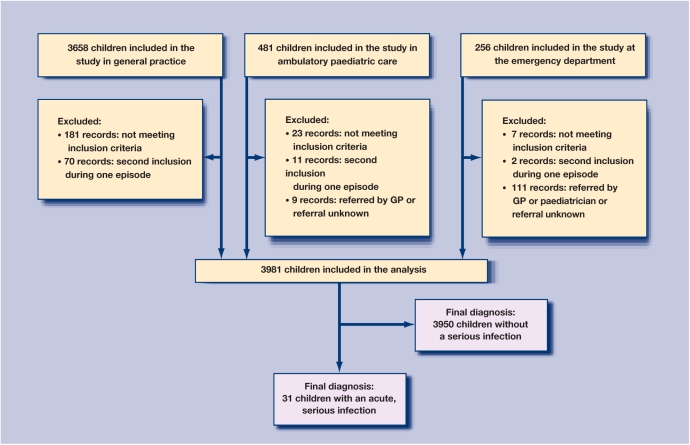
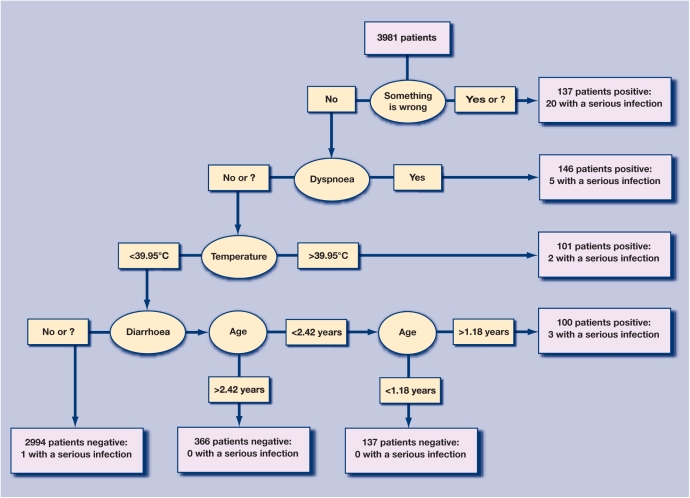
Method: Children aged 0-16 years with an acute illness for a maximum of 5 days were included consecutively. Signs and symptoms were recorded and compared to the final outcome of these children (a serious infection for which hospitalisation was necessary). Accuracy was analysed bivariably. Multivariable triage instruments were constructed using classification and regression tree (CART) analysis.
Results: A total of 3981 children were included in the study, of which 31 were admitted to hospital with a serious infection (0.78%). Accuracy of signs and symptoms was fairly low. Classical textbook signs (meningeal irritation impaired peripheral circulation) had high specificity. The primary classification tree consisted of five knots and had sensitivity of 96.8% (95% confidence interval [CI] = 83.3 to 99.9), specificity 88.5% (95% CI = 87.5 to 89.5), positive predictive value 6.2% (95% CI = 4.2 to 8.7), and negative predictive value 100.0% (95% CI = 99.8 to 100.0), by which a serious infection can be excluded in children testing negative on the tree. The sign paramount in all trees was the physician's statement 'something is wrong'.
Conclusion: Some individual signs have high specificity. A serious infection can be excluded based on a limited number of signs and symptoms.
Figures
References
-
- Bleeker SE, et al. Predicting serious bacterial infection in young children with fever without apparent source. Acta Paediatr. 2001;90:1226–1232. - PubMed
-
- Koomen I, et al. Hearing loss at school age in survivors of bacterial meningitis: assessment, incidence, and prediction. Pediatrics. 2003;112:1049–1053. - PubMed
-
- Care-and-health. The Flemish agency for care and health, (agency of the Flemish ministry for health and family) http://www.zorg-en-gezondheid.be (accessed 7 Jun 2007)
-
- Wilson D. Impact of infection on mortality and hospitalization in the North East of England. J Public Health Med. 1998;20:386–395. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials