

Laparoscopic myomectomy for large myomas
- PMID: 17728514
- PMCID: PMC2693824
- DOI: 10.3346/jkms.2007.22.4.706
Laparoscopic myomectomy for large myomas
Abstract
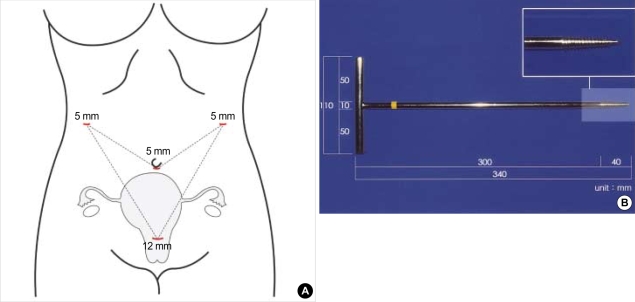
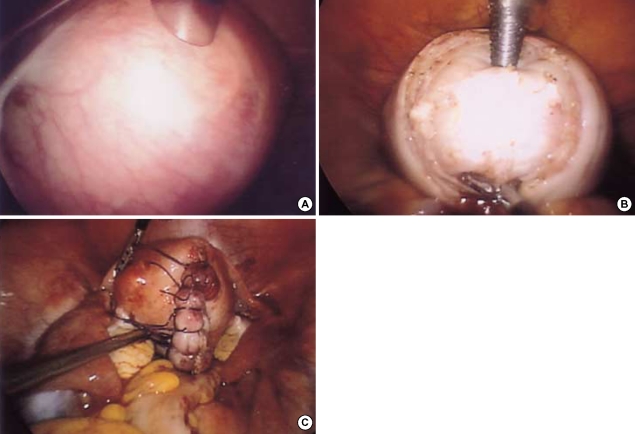
The aim of this study was to assess the feasibility and efficacy of laparoscopic myomectomy (LM) for large myomas. A subpopulation of 51 patients with myomas 8 cm or larger in diameter was selected from 155 patients who underwent LM at Kangbuk Samsung Hospital from July 2003 to November 2006. The mean age of the patients was 34.9 +/- 5.6 yr, mean parity was 0.6 +/- 0.9, and 8 patients had a previous operative history. The most common operative indication was a palpable abdominal mass (24 patients, 47%). The mean operating time was 85.6 +/- 38.9 min, and the mean diameter of the largest myoma was 9.3 +/- 1.8 cm. The mean change in hemoglobin concentration was 2.1 +/- 1.2 g/dL. Histopathological diagnosis included 49 patients of leiomyoma (96.1%) and 2 patients of leiomyoma with adenomyosis (3.9%). Postoperatively, a transfusion was done in 7 patients, and a case of subcutaneous emphysema was noted. None of the operations was switched to laparotomy. With the newly-developed screw and the port placement system that was modified from the Choi's 4-trocar method to obtain better surgical vision, LM of large myomas proved to be one of the efficient and feasible methods.
Figures
Similar articles
-
Surgical outcomes of a new approach to laparoscopic myomectomy: single-port and modified suture technique.J Minim Invasive Gynecol. 2014 Jul-Aug;21(4):580-5. doi: 10.1016/j.jmig.2013.12.096. Epub 2013 Dec 31. J Minim Invasive Gynecol. 2014. PMID: 24384072
-
Laparoendoscopic single-site myomectomy compared with conventional laparoscopic myomectomy: a multicenter, randomized, controlled trial.Fertil Steril. 2015 Nov;104(5):1325-31. doi: 10.1016/j.fertnstert.2015.07.1137. Epub 2015 Aug 8. Fertil Steril. 2015. PMID: 26263079 Clinical Trial.
-
Single port laparoscopic myomectomy with intracorporeal suture-tying and transumbilical morcellation.Eur J Obstet Gynecol Reprod Biol. 2014 Oct;181:200-4. doi: 10.1016/j.ejogrb.2014.07.051. Epub 2014 Aug 8. Eur J Obstet Gynecol Reprod Biol. 2014. PMID: 25150961
-
[Laparoscopic surgery of large uterine fibromas. Operative technique and results].J Gynecol Obstet Biol Reprod (Paris). 1995;24(7):705-10. J Gynecol Obstet Biol Reprod (Paris). 1995. PMID: 8568177 Review. French.
-
[Laparoscopic myomectomy in 2007: state of the art].J Gynecol Obstet Biol Reprod (Paris). 2007 Oct;36(6):567-76. doi: 10.1016/j.jgyn.2007.05.003. Epub 2007 Jun 26. J Gynecol Obstet Biol Reprod (Paris). 2007. PMID: 17597308 Review. French.
Cited by
-
Successful use of laparoscopic myomectomy to remove a giant uterine myoma: a case report.J Med Case Rep. 2015 Dec 17;9:286. doi: 10.1186/s13256-015-0771-9. J Med Case Rep. 2015. PMID: 26674527 Free PMC article.
-
Predictors of postoperative hemoglobin drop after laparoscopic myomectomy.Wideochir Inne Tech Maloinwazyjne. 2017;12(1):81-87. doi: 10.5114/wiitm.2017.66515. Epub 2017 Mar 13. Wideochir Inne Tech Maloinwazyjne. 2017. PMID: 28446936 Free PMC article.
-
Feasibility of Laparoscopic Removal of the Largest Documented Uterine Fibroid Without Morcellation.Reports (MDPI). 2025 May 17;8(2):71. doi: 10.3390/reports8020071. Reports (MDPI). 2025. PMID: 40710862 Free PMC article.
-
Pushing the boundaries of laparoscopic myomectomy: a comparative analysis of peri-operative outcomes in 323 women undergoing laparoscopic myomectomy in a tertiary referral centre.Gynecol Surg. 2017;14(1):22. doi: 10.1186/s10397-017-1025-1. Epub 2017 Nov 13. Gynecol Surg. 2017. PMID: 29200989 Free PMC article.
-
The prevalence of occult leiomyosarcoma at surgery for presumed uterine fibroids: a meta-analysis.Gynecol Surg. 2015;12(3):165-177. doi: 10.1007/s10397-015-0894-4. Epub 2015 May 19. Gynecol Surg. 2015. PMID: 26283890 Free PMC article. Review.
References
-
- Hurst BS, Matthews ML, Marshburn PB. Laparoscopic myomectomy for symptomatic uterine myomas. Fertil Steril. 2005;83:1–23. - PubMed
-
- Alessandri F, Lijoi D, Mistrangelo E, Ferrero S, Ragni N. Randomized study of laparoscopic versus minilaparotomic myomectomy for uterine myomas. J Minim Invasive Gynecol. 2006;13:92–97. - PubMed
-
- Sinha R, Hegde A, Warty N, Patil N. Laparoscopic excision of very large myomas. J Am Assoc Gynecol Laparosc. 2003;10:461–468. - PubMed
-
- Marret H, Chevillot M, Giraudeau B. Factors influencing laparoconversions during the learning curve of laparoscopic myomectomy. Acta Obstet Gynecol Scand. 2006;85:324–329. - PubMed
-
- Marret H, Chevillot M, Giraudeau B. A retrospective multicentre study comparing myomectomy by laparoscopy and laparotomy in current surgical practice. What are the best patient selection criteria? Eur J Obstet Gynecol Reprod Biol. 2004;117:82–86. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
