

Accessibility, clinical effectiveness, and practice costs of providing a telephone option for routine asthma reviews: phase IV controlled implementation study
- PMID: 17761059
- PMCID: PMC2151786
Accessibility, clinical effectiveness, and practice costs of providing a telephone option for routine asthma reviews: phase IV controlled implementation study
Abstract
Background: Attendance for routine asthma reviews is poor. A recent randomised controlled trial found that telephone consultations can cost-effectively and safely enhance asthma review rates; however, concerns have been expressed about the generalisability and implementation of the trial's findings.
Aim: To evaluate the effectiveness of a telephone option as part of a routine structured asthma review service.
Design of study: Phase IV controlled before-and-after implementation study.
Setting: A large UK general practice.
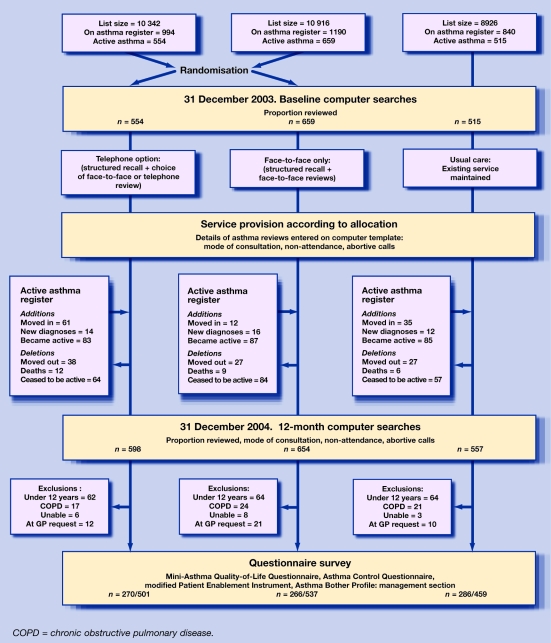
Method: Using existing administrative groups, all patients with active asthma (n = 1809) received one of three asthma review services: structured recall with a telephone-option for reviews versus structured recall with face-to-face-only reviews, or usual-care (to assess secular trends). Main outcome measures were: proportion of patients with active asthma reviewed within the previous 15 months (Quality and Outcomes Framework target), mode of review, enablement, morbidity, and costs to the practice.
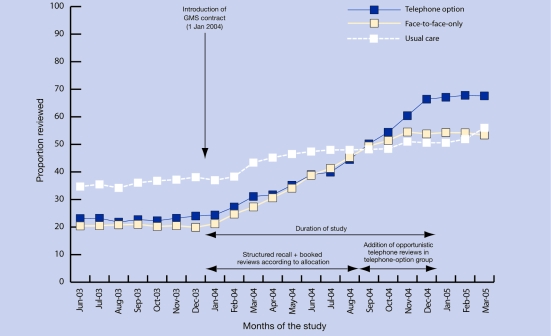
Results: A routine asthma review was provided for 397/598 (66.4%) patients in the telephone-option group compared with 352/654 (53.8%) in the face-to-face-only review group: risk difference 12.6% (95% confidence interval [CI] = 7.2 to 17.9, P<0.001). The usual-care group achieved a review rate of 282/557 (50.6%). Morbidity was equivalent in the three groups; however, enablement (P = 0.03) and confidence (P = 0.007) in asthma management were greater in the telephone-option versus face-to-face-only group. The cost per review achieved by providing the telephone-option service was lower than the face-to-face-only service (10.03 pounds versus 12.74 pounds, mean difference 2.71 pounds; 95% CI = 1.92 to 3.50, P<0.001); usual-care costs were 11.85 pounds per review achieved.
Conclusion: Routinely offering telephone reviews cost-effectively increased asthma review rates, enhancing patient enablement and confidence with management, with no detriment to asthma morbidity. Practices should consider a telephone option for their asthma review service.
Figures
References
-
- General Medical Council. Good medical practice. 3rd edn. London: General Medical Council; 2001.
-
- Gruffydd-Jones K, Nicholson I, Best L, Connell E. Asthma in general practice. Why don't patients attend the asthma clinic? Asthma Gen Pract. 1999;7:36–39.
-
- Price D, Wolfe S. Delivery of asthma care: patient's use of and views on healthcare services, as determined from a nationwide interview survey. Asthma J. 2000;5:141–144.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials