

Implications of method specific creatinine adjustments on General Medical Services chronic kidney disease classification
- PMID: 17761741
- PMCID: PMC1972412
- DOI: 10.1136/jcp.2006.043547
Implications of method specific creatinine adjustments on General Medical Services chronic kidney disease classification
Abstract
Aims: To evaluate the impact of different equations for calculation of estimated glomerular filtration rate (eGFR) on general practitioner (GP) workload.
Methods: Retrospective evaluation of routine workload data from a district general hospital chemical pathology laboratory serving a GP patient population of approximately 250 000. The most recent serum creatinine result from 80 583 patients was identified and used for the evaluation. eGFR was calculated using one of three different variants of the four-parameter Modification of Diet in Renal Disease (MDRD) equation.
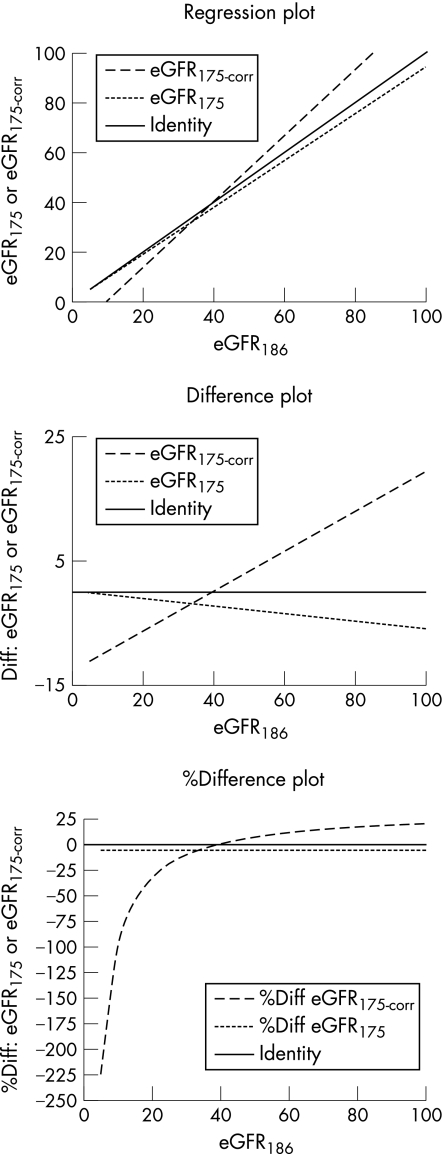
Results: The original MDRD equation (eGFR(186)) and the modified equation with assay-specific data (eGFR(175corrected)) both identified similar numbers of patients with stage 4 and stage 5 chronic kidney disease (ChKD), but the modified equation without assay specific data (eGFR(175)) resulted in a significant increase in stage 4 ChKD. For stage 3 ChKD the eGFR(175) identified 28.69% of the population, the eGFR(186) identified 21.35% of the population and the eGFR(175corrected) identified 13.6% of the population.
Conclusions: Depending on the choice of equation there can be very large changes in the proportions of patients identified with the different stages of ChKD. Given that according to the General Medical Services Quality Framework, all patients with ChKD stages 3-5 should be included on a practice renal registry, and receive relevant drug therapy, this could have significant impacts on practice workload and drug budgets. It is essential that practices work with their local laboratories.
Conflict of interest statement
Competing interests: None.
Similar articles
-
Impact of routine reporting of estimated glomerular filtration rate using the CKD-EPI formula in a community population: A cross-sectional cohort study.Nephrology (Carlton). 2014 Sep;19(9):581-6. doi: 10.1111/nep.12283. Nephrology (Carlton). 2014. PMID: 24888643
-
The Chronic Kidney Disease Epidemiology Collaboration cystatin C (CKD-EPI-CysC) equation has an independent prognostic value for overall survival in newly diagnosed patients with symptomatic multiple myeloma; is it time to change from MDRD to CKD-EPI-CysC equations?Eur J Haematol. 2013 Oct;91(4):347-55. doi: 10.1111/ejh.12164. Epub 2013 Aug 17. Eur J Haematol. 2013. PMID: 23829647
-
Estimated Glomerular Filtration Rate; Laboratory Implementation and Current Global Status.Adv Chronic Kidney Dis. 2018 Jan;25(1):7-13. doi: 10.1053/j.ackd.2017.09.013. Adv Chronic Kidney Dis. 2018. PMID: 29499890 Review.
-
Enzymatic creatinine assays allow estimation of glomerular filtration rate in stages 1 and 2 chronic kidney disease using CKD-EPI equation.Clin Chim Acta. 2014 Jan 20;428:89-95. doi: 10.1016/j.cca.2013.11.002. Epub 2013 Nov 10. Clin Chim Acta. 2014. PMID: 24220551
-
GFR estimation: from physiology to public health.Am J Kidney Dis. 2014 May;63(5):820-34. doi: 10.1053/j.ajkd.2013.12.006. Epub 2014 Jan 28. Am J Kidney Dis. 2014. PMID: 24485147 Free PMC article. Review.
Cited by
-
The four-variable modification of diet in renal disease formula underestimates glomerular filtration rate in obese type 2 diabetic individuals with chronic kidney disease.Diabetologia. 2011 Jun;54(6):1304-7. doi: 10.1007/s00125-011-2085-9. Epub 2011 Feb 26. Diabetologia. 2011. PMID: 21359581
-
Best practice in primary care pathology: review 10.J Clin Pathol. 2007 Nov;60(11):1195-204. doi: 10.1136/jcp.2007.048512. Epub 2007 May 11. J Clin Pathol. 2007. PMID: 17496187 Free PMC article. Review.
-
Visceral Adiposity as an Independent Risk Factor for Diabetic Peripheral Neuropathy in Type 2 Diabetes Mellitus: A Retrospective Study.J Diabetes Res. 2024 Nov 11;2024:9912907. doi: 10.1155/2024/9912907. eCollection 2024. J Diabetes Res. 2024. PMID: 39559714 Free PMC article.
References
-
- National Kidney Foundation Kidney Disease Outcomes Quality Initiative K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: Evaluation, classification, and stratification. American Journal of Kidney Diseases 200239(2)S7–266. - PubMed
-
- Levey A S, Greene T, Kusek J W.et al A simplified equation to predict glomerular filtration rate from serum creatinine [abstract]. J Am Soc Nephrol 200011A0828
-
- National Kidney Disease Education Program (NKDEP) Suggestions for laboratories (December 2005). http://www.nkdep.nih.gov/resources/laboratory_reporting.htm (accessed 1 June 2006)
-
- Mackenzie F. UKNEQAS of GFR estimations [pilot]. http://www.ukneqas.org.uk/GFR%20Estimations.pdf (accessed 1 June 2006)
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous