

Perceptions of surgical specialists in general surgery, orthopaedic surgery, urology and gynaecology on teaching endoscopic surgery in The Netherlands
- PMID: 17762954
- PMCID: PMC2234445
- DOI: 10.1007/s00464-007-9491-6
Perceptions of surgical specialists in general surgery, orthopaedic surgery, urology and gynaecology on teaching endoscopic surgery in The Netherlands
Abstract
Background: Specific training in endoscopic skills and procedures has become a necessity for profession with embedded endoscopic techniques in their surgical palette. Previous research indicates endoscopic skills training to be inadequate, both from subjective (resident interviews) and objective (skills measurement) viewpoint. Surprisingly, possible shortcomings in endoscopic resident education have never been measured from the perspective of those individuals responsible for resident training, e.g. the program directors. Therefore, a nation-wide survey was conducted to inventory current endoscopic training initiatives and its possible shortcomings among all program directors of the surgical specialties in the Netherlands.
Methods: Program directors for general surgery, orthopaedic surgery, gynaecology and urology were surveyed using a validated 25-item questionnaire.
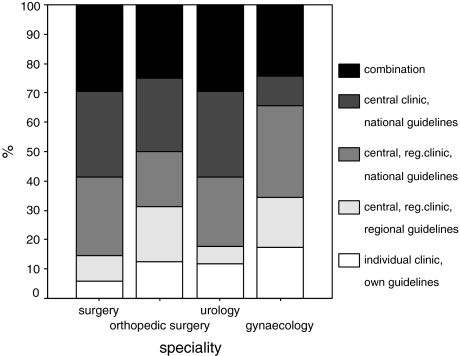
Results: A total of 113 program directors responded (79%). The respective response percentages were 73.6% for general surgeons, 75% for orthopaedic surgeon, 90.9% for urologists and 68.2% for gynaecologists. According to the findings, 35% of general surgeons were concerned about whether residents are properly skilled endoscopically upon completion of training. Among the respondents, 34.6% were unaware of endoscopic training initiatives. The general and orthopaedic surgeons who were aware of these initiatives estimated the number of training hours to be satisfactory, whereas the urologists and gynaecologists estimated training time to be unsatisfactory. Type and duration of endoscopic skill training appears to be heterogeneous, both within and between the specialties. Program directors all perceive virtual reality simulation to be a highly effective training method, and a multimodality training approach to be key. Respondents agree that endoscopic skills education should ideally be coordinated according to national consensus and guidelines.
Conclusions: A delicate balance exists between training hours and clinical working hours during residency. Primarily, a re-allocation of available training hours, aimed at core-endoscopic basic and advanced procedures, tailored to the needs of the resident and his or her phase of training is in place. The professions need to define which basic and advanced endoscopic procedures are to be trained, by whom, and by what outcome standards. According to the majority of program directors, virtual reality (VR) training needs to be integrated in procedural endoscopic training courses.
Figures













Similar articles
-
Current and future use of surgical skills training laboratories in orthopaedic resident education: a national survey.J Bone Joint Surg Am. 2013 Jan 2;95(1):e4. doi: 10.2106/JBJS.L.00177. J Bone Joint Surg Am. 2013. PMID: 23283381
-
Managing expectations of surgical training: a national perspective on gynaecologic endoscopy practice.J Obstet Gynaecol Can. 2013 Jul;35(7):640-646. doi: 10.1016/S1701-2163(15)30892-6. J Obstet Gynaecol Can. 2013. PMID: 23876642
-
Necessity for improvement in endoscopy training during surgical residency.Am J Surg. 2010 Mar;199(3):331-4; discussion 334-5. doi: 10.1016/j.amjsurg.2009.09.013. Am J Surg. 2010. PMID: 20226905
-
Overview of methods for flexible endoscopic training and description of a simple explant model.Asian J Endosc Surg. 2011 May;4(2):45-52. doi: 10.1111/j.1758-5910.2011.00078.x. Epub 2011 Mar 17. Asian J Endosc Surg. 2011. PMID: 22776220 Review.
-
A Review of Endoscopic Simulation: Current Evidence on Simulators and Curricula.J Surg Educ. 2016 Jan-Feb;73(1):12-23. doi: 10.1016/j.jsurg.2015.09.001. Epub 2015 Dec 11. J Surg Educ. 2016. PMID: 26699281 Review.
Cited by
-
Measuring learning gain during a one-day introductory bronchoscopy course.Surg Endosc. 2011 Jan;25(1):207-16. doi: 10.1007/s00464-010-1161-4. Epub 2010 Jun 29. Surg Endosc. 2011. PMID: 20585964 Free PMC article.
-
Pressure-dependent hydrometra dimensions in hysteroscopy.Surg Endosc. 2009 Sep;23(9):2102-9. doi: 10.1007/s00464-008-0231-3. Epub 2008 Dec 6. Surg Endosc. 2009. PMID: 19067060
-
Resident training in minimally invasive surgery: a survey of Canadian department and division chairs.Surg Endosc. 2010 Mar;24(3):499-503. doi: 10.1007/s00464-009-0611-3. Epub 2009 Jul 8. Surg Endosc. 2010. PMID: 19585067
-
Problems and pitfalls in modern competency-based laparoscopic training.Surg Endosc. 2011 Jul;25(7):2159-63. doi: 10.1007/s00464-010-1515-y. Epub 2011 Feb 7. Surg Endosc. 2011. PMID: 21298547 Free PMC article. No abstract available.
-
Procedural virtual reality simulation in minimally invasive surgery.Surg Endosc. 2013 Feb;27(2):364-77. doi: 10.1007/s00464-012-2503-1. Epub 2012 Sep 7. Surg Endosc. 2013. PMID: 22956001 Review.
References
-
- Sauerland S, Agresta F, Bergamaschi R, Borzellino G, Budzynski A, Champault G, Fingerhut A, Isla A, Johansson M, Lundorff P, et al. Laparoscopy for abdominal emergencies: evidence-based guidelines of the European Association for Endoscopic Surgery. Surg Endosc. 2006;20(1):14–29. doi: 10.1007/s00464-005-0564-0. - DOI - PubMed
-
- American society of colon, rectal surgeons (ASCRS) gastrointestinal and endoscopic surgeons (SAGES) Fleshman J, Marcello P, Stamos MJ, Wexner S. Focus Group on Laparoscopic Colectomy Education as endorsed by the American Society of Colon and Rectal Surgeons (ASCRS) and the Society of American Gastrointestinal and Endoscopic Surgeons (SAGES): guidelines for laparoscopic colectomy course. Surg Endosc. 2006;20(7):1162–1167. doi: 10.1007/s00464-006-0212-3. - DOI - PubMed
-
- no authors listed: (1999) Guidelines for diagnostic laparoscopy. SAGES guidelines. Society of American Gastrointestinal Endoscopic Surgeons. Surg Endosc 13(2):202–203 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
