

Serious infection following anti-tumor necrosis factor alpha therapy in patients with rheumatoid arthritis: lessons from interpreting data from observational studies
- PMID: 17763441
- PMCID: PMC2435418
- DOI: 10.1002/art.22808
Serious infection following anti-tumor necrosis factor alpha therapy in patients with rheumatoid arthritis: lessons from interpreting data from observational studies
Abstract
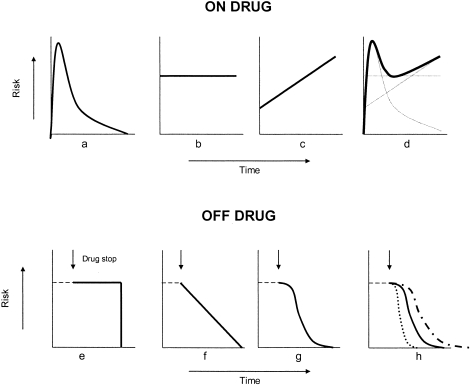
Objective: In a recent observational study, we found that the risk of serious infection following anti-tumor necrosis factor alpha (anti-TNFalpha) therapy in patients with rheumatoid arthritis (RA) was not importantly increased compared with the background risk in routinely treated RA patients with similar disease severity. Observational data sets are, however, subject to a number of important biases related to selection factors for the timing of starting and stopping therapy. Infection risk is also likely to vary with duration of therapy. This study was undertaken to examine the influences of these biases and of the method of analysis on the risk of infection.
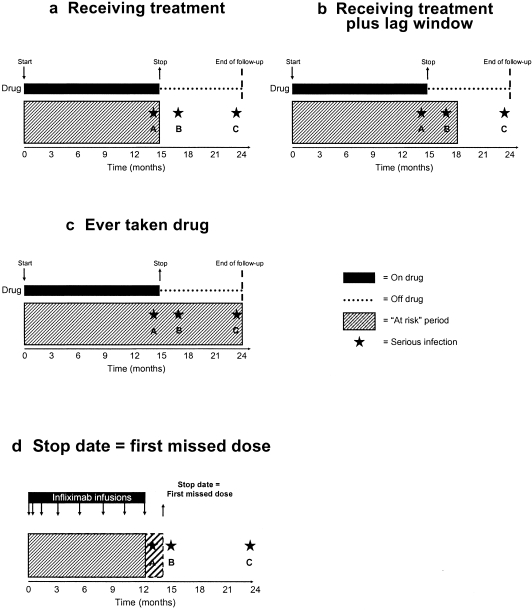
Methods: We compared the risk of serious infection in 8,659 patients treated with anti-TNFalpha with that in 2,170 patients treated with traditional disease-modifying antirheumatic drugs (DMARDs) recruited to the British Society for Rheumatology Biologics Register. We applied a number of statistical models in which we varied the length of the followup period by using different definitions of the date of discontinuation of treatment and different lag periods of risk following drug cessation.
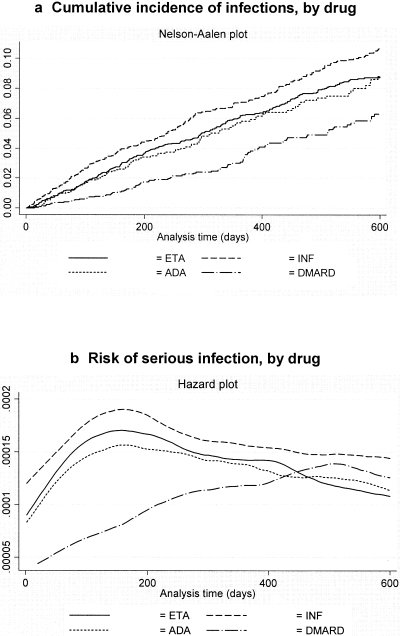
Results: When the at-risk period was defined as "receiving treatment", the adjusted incidence rate ratio comparing patients receiving anti-TNFalpha therapy with patients receiving DMARD therapy was 1.22 (95% confidence interval [95% CI] 0.88-1.69). Limiting followup to the first 90 days, however, revealed an adjusted incidence rate ratio of 4.6 (95% CI 1.8-11.9). Rates of infection were increased in the 90 days immediately following drug discontinuation and beyond, explained by selection factors for drug discontinuation.
Conclusion: These findings show that overall, the way in which UK rheumatologists select patients for starting and discontinuing anti-TNFalpha therapy explains our previous finding of no increase in risk. However, there may be important increases in true risk, notably early in the course of treatment, that would become more evident depending on the definition of at-risk period.
Figures
References
-
- Listing J, Strangfeld A, Kary S, Rau R, von Hinueber U, Stoyanova-Scholz M, et al. Infections in patients with rheumatoid arthritis treated with biologic agents. Arthritis Rheum. 2005;52:3403–12. - PubMed
-
- Dixon WG, Watson K, Lunt M, Hyrich KL, Silman AJ, British Society for Rheumatology Biologics Register Control Centre Consortium et al. on behalf of the British Society for Rheumatology Biologics Register Rates of serious infection, including site-specific and bacterial intracellular infection, in rheumatoid arthritis patients receiving anti–tumor necrosis factor therapy: results from the British Society for Rheumatology Biologics Register. Arthritis Rheum. 2006;54:2368–76. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
