

Physicians' views on resource availability and equity in four European health care systems
- PMID: 17764556
- PMCID: PMC1995213
- DOI: 10.1186/1472-6963-7-137
Physicians' views on resource availability and equity in four European health care systems
Abstract
Background: In response to limited resources, health care systems have adopted diverse cost-containment strategies and give priority to differing types of interventions. The perception of physicians, who witness the effects of these strategies, may provide useful insights regarding the impact of system-wide priority setting on access to care.
Methods: We conducted a cross-sectional survey to ascertain generalist physicians' perspectives on resources allocation and its consequences in Norway, Switzerland, Italy and the UK.
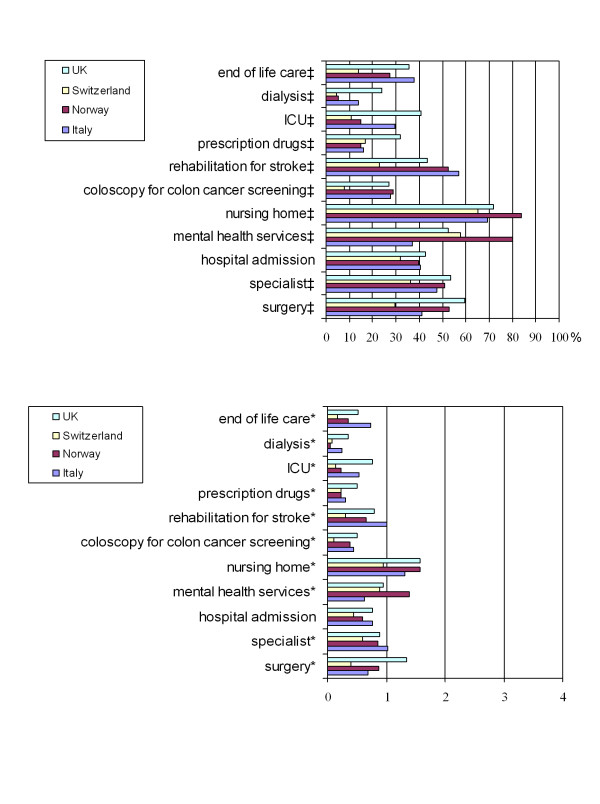
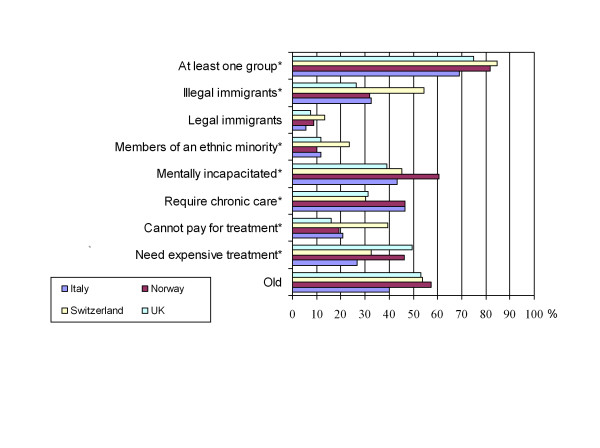
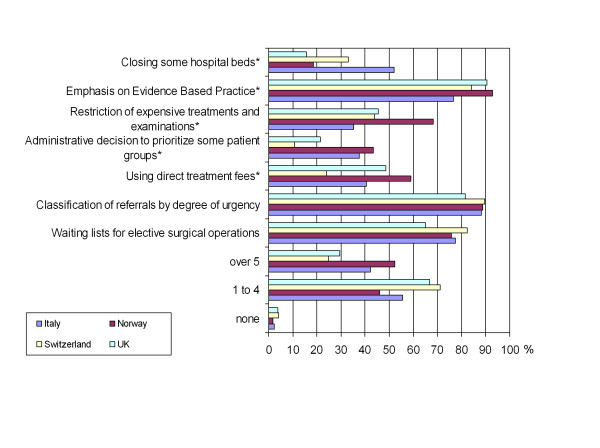
Results: Survey respondents (N = 656, response rate 43%) ranged in age from 28-82, and averaged 25 years in practice. Most respondents (87.7%) perceived some resources as scarce, with the most restrictive being: access to nursing home, mental health services, referral to a specialist, and rehabilitation for stroke. Respondents attributed adverse outcomes to scarcity, and some respondents had encountered severe adverse events such as death or permanent disability. Despite universal coverage, 45.6% of respondents reported instances of underinsurance. Most respondents (78.7%) also reported some patient groups as more likely than others to be denied beneficial care on the basis of cost. Almost all respondents (97.3%) found at least one cost-containment policy acceptable. The types of policies preferred suggest that respondents are willing to participate in cost-containment, and do not want to be guided by administrative rules (11.2%) or restrictions on hospital beds (10.7%).
Conclusion: Physician reports can provide an indication of how organizational factors may affect availability and equity of health care services. Physicians are willing to participate in cost-containment decisions, rather than be guided by administrative rules. Tools should be developed to enable physicians, who are in a unique position to observe unequal access or discrimination in their health care environment, to address these issues in a more targeted way.
Figures
References
-
- Aaron HJ, Schwartz WB. Studies in Social Economics. Washington D.C. , The Brookings Institution; 1984. The Painful Prescription; Rationing Hospital Care.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
