

Permanent tracheostomy for long-term respiratory studies
- PMID: 17764697
- PMCID: PMC2277486
- DOI: 10.1016/j.jss.2007.03.076
Permanent tracheostomy for long-term respiratory studies
Abstract
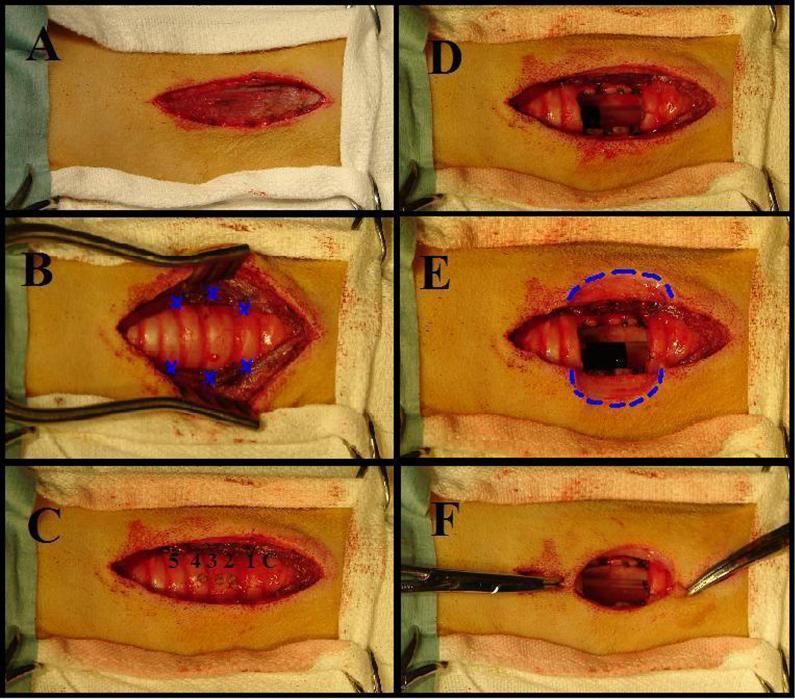
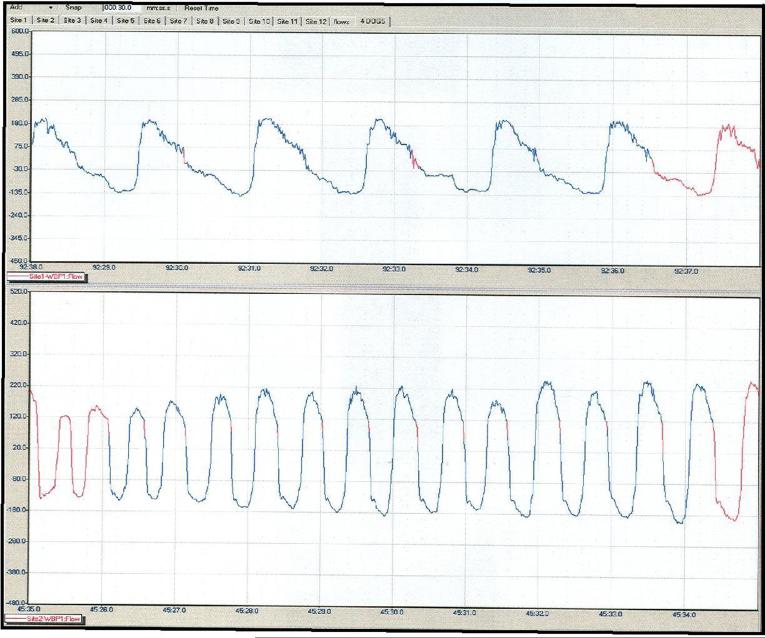
Background: We describe a modified surgical technique for permanent, anterior tracheal-wall stoma for chronic, repeat respiratory studies in trained, conscious dogs. These cannula-free tracheostomies require minimal daily maintenance, permit repeat intubation with endotracheal tubes modified for airflow respiratory measurement, and facilitate up to 6 h continuous administration of aerosol agents during long-term or repeat respiratory studies.
Methods: In 20 dogs, during a 30 to 40 min procedure, portions of tracheal rings 2-4 were removed to create an oval stoma, approximately 2 x 1 cm. The dermis was secured to the transected cartilage and tracheal mucosa in such a manner that skin covered the sternohyoid muscles and grew-in flush with the tracheal mucosa at the stomal opening. Stomas were cleaned daily, and fur was clipped weekly around the stomal site. No other maintenance procedures or environmental modifications were needed. Animals breathed through both the stoma and the upper airway and barked normally.
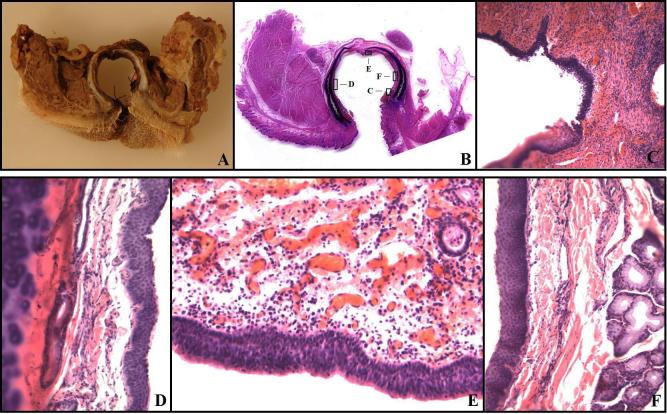
Results: Stomas remained viable in long-term animals (n = 4) ongoing for 70.3 +/- 32.2 mo (mean +/- SEM), with an ongoing maximum of 126 mo. Postmortem examinations were performed on shorter-term animals (n = 16) sacrificed at 16.7 +/- 7.3 mo. Thirteen showed no appreciable tracheal stenosis and three showed <10% stenosis at the level of the stoma. Histopathological examination of the stomal opening and surrounding tissue revealed minimal chronic inflammation and no evidence of necrosis or infection.
Conclusions: During long-term respiratory studies, this practical and dependable tracheal stoma provides a means for examining acute and chronic effects of environmental and pathophysiological influences on the respiratory system of conscious dogs.
Figures

References
-
- Foss ML, Barnard RJ, Tipton CM. Use of tracheostomized dogs in chronic metabolic assessments of treadmill work. Lab Anim Sci. 1972 Jun;22(3):397–401. - PubMed
-
- Murphy DA, MacLean LD, Dobell AR. Tracheal stenosis as a complication of tracheostomy. Ann Thorac Surg. 1966 Jan;2(1):44–51. - PubMed
-
- Ching NP, Ayres SM, Paegle RP, Linden JM, Nealon TF., Jr The contribution of cuff volume and pressure in tracheostomy tube damage. J Thorac Cardiovasc Surg. 1971 Sep;62(3):402–10. - PubMed
-
- Shelly WM, Dawson RB, May IA. Cuffed tubes as a cause of tracheal stenosis. J Thorac Cardiovasc Surg. 1969 May;57(5):623–7. - PubMed
-
- Mendez-Picon G, Ehrlich FE, Salzberg AM. The effect of tracheostomy incisions on tracheal growth. J Pediatr Surg. 1976 Oct;11(5):681–5. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
