

JAK2V617F-negative ET patients do not display constitutively active JAK/STAT signaling
- PMID: 17764814
- PMCID: PMC2270411
- DOI: 10.1016/j.exphem.2007.07.004
JAK2V617F-negative ET patients do not display constitutively active JAK/STAT signaling
Abstract
Objective: Presence of the JAK2V617F mutation in only 40% to 60% of patients with essential thrombocythemia (ET) underscores the heterogeneity of this myeloproliferative disorder (MPD). Several distinct mutations, either in JAK2 (exon 12) or in c-Mpl (W515L) have been described in subsets of other MPDs, polycythemia vera, and idiopathic myelofibrosis. Analogous to JAK2,V617F these mutations cause constitutive JAK2 and signal transducer and activation of transcription (STAT) activation. It has therefore been proposed that constitutive activation of the JAK/STAT pathway underlies the molecular etiology of all MPDs. We investigated the alternative hypothesis that distinct alterations, separate from the JAK/STAT signal transduction pathway, underlie a subset of JAK2V617F-negative ET.
Methods: cDNA microarrays and quantitative reverse transcriptase polymerase chain reactions were used to compare gene expression in 40 ET patients with and without the JAK2V617F mutation.
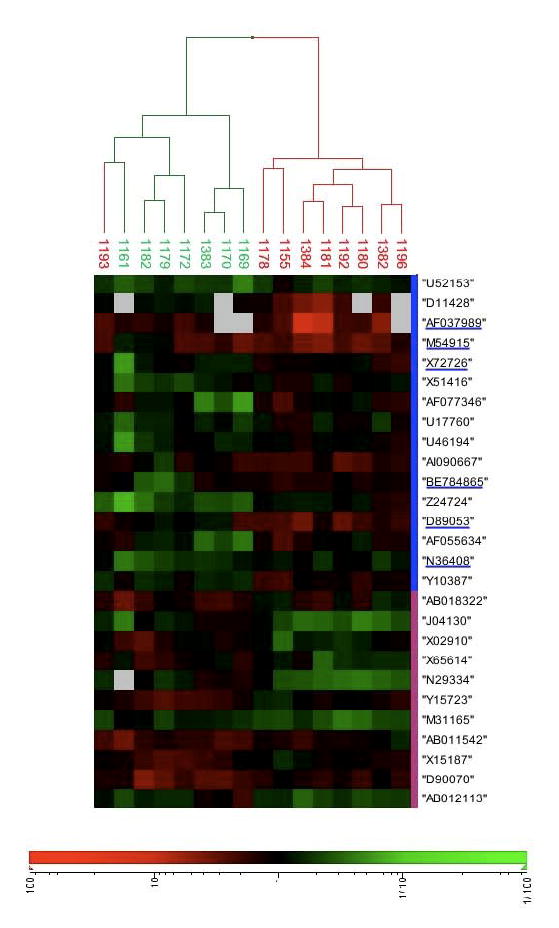
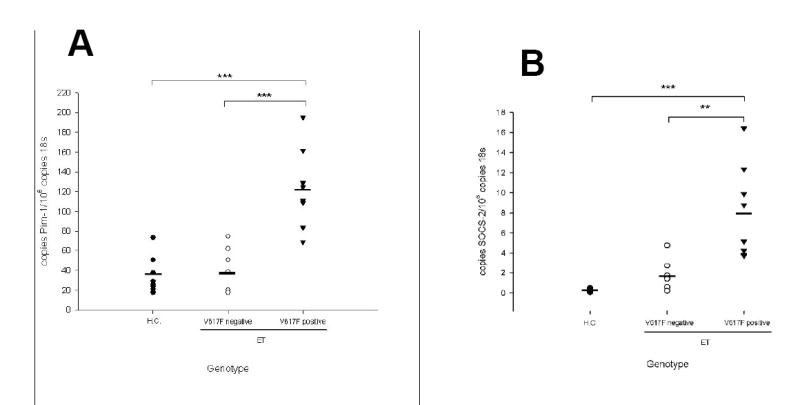
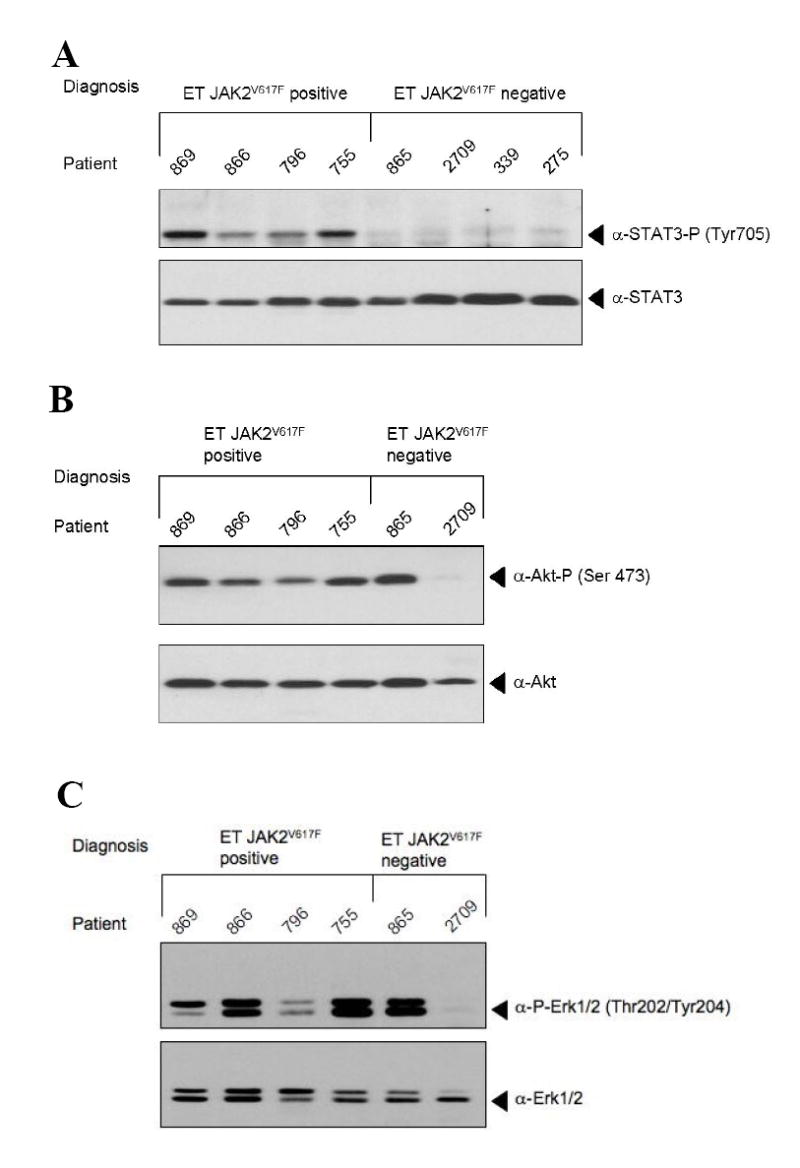
Results: Unsupervised clustering of gene-expression patterns in ET patients revealed two distinct subclasses of patients. These subclasses differed in presence or absence of the JAK2V617F mutation. Patients lacking the JAK2V617F mutation displayed significantly lower expression of the JAK/STAT target genes Pim-1 and suppressor of cytokine signaling-2. In addition, JAK2V617F-negative patients showed lower levels of STAT3 phosphorylation.
Conclusions: These data demonstrate that a large proportion of JAK2V617F-negative ET patients do not display constitutive JAK/STAT signaling. Hence, we propose that alterations in different signal transduction pathways can lead to the clinical phenotype of ET. Elucidation of novel ET-inducing changes will facilitate both a molecular classification of ET and development of rationally designed therapies.
Figures

Similar articles
-
Role of JAK-STAT signaling in the pathogenesis of myeloproliferative disorders.Hematology Am Soc Hematol Educ Program. 2006:233-9, 510. doi: 10.1182/asheducation-2006.1.233. Hematology Am Soc Hematol Educ Program. 2006. PMID: 17124066 Review.
-
Essential thrombocythaemia progression to the fibrotic phase is associated with a decrease in JAK2 and PDL1 levels.Ann Hematol. 2022 Dec;101(12):2665-2677. doi: 10.1007/s00277-022-05001-8. Epub 2022 Oct 21. Ann Hematol. 2022. PMID: 36266510 Free PMC article.
-
MPLW515L is a novel somatic activating mutation in myelofibrosis with myeloid metaplasia.PLoS Med. 2006 Jul;3(7):e270. doi: 10.1371/journal.pmed.0030270. PLoS Med. 2006. PMID: 16834459 Free PMC article.
-
Different STAT-3 and STAT-5 phosphorylation discriminates among Ph-negative chronic myeloproliferative diseases and is independent of the V617F JAK-2 mutation.Blood. 2007 Jul 1;110(1):354-9. doi: 10.1182/blood-2007-01-069237. Epub 2007 Mar 21. Blood. 2007. PMID: 17376889
-
JAK2 and MPL mutations in myeloproliferative neoplasms: discovery and science.Leukemia. 2008 Oct;22(10):1813-7. doi: 10.1038/leu.2008.229. Epub 2008 Aug 28. Leukemia. 2008. PMID: 18754026 Review.
Cited by
-
Targeting Pim kinases in hematological cancers: molecular and clinical review.Mol Cancer. 2023 Jan 25;22(1):18. doi: 10.1186/s12943-023-01721-1. Mol Cancer. 2023. PMID: 36694243 Free PMC article. Review.
-
From oncoproteins/tumor suppressors to microRNAs, the newest therapeutic targets for pulmonary arterial hypertension.J Mol Med (Berl). 2011 Nov;89(11):1089-101. doi: 10.1007/s00109-011-0788-5. Epub 2011 Jul 15. J Mol Med (Berl). 2011. PMID: 21761156 Review.
-
Mass cytometry analysis reveals hyperactive NF Kappa B signaling in myelofibrosis and secondary acute myeloid leukemia.Leukemia. 2017 Sep;31(9):1962-1974. doi: 10.1038/leu.2016.377. Epub 2016 Dec 23. Leukemia. 2017. PMID: 28008177 Free PMC article.
-
Stat5 Exerts Distinct, Vital Functions in the Cytoplasm and Nucleus of Bcr-Abl+ K562 and Jak2(V617F)+ HEL Leukemia Cells.Cancers (Basel). 2015 Mar 19;7(1):503-37. doi: 10.3390/cancers7010503. Cancers (Basel). 2015. PMID: 25809097 Free PMC article.
-
IL-6 stimulation of DNA replication is JAK1/2 mediated in cross-talk with hyperactivated ERK1/2 signaling.Cell Biol Int. 2019 Feb;43(2):192-206. doi: 10.1002/cbin.11084. Epub 2019 Jan 7. Cell Biol Int. 2019. PMID: 30571852 Free PMC article.
References
-
- Gisslinger H. Update on diagnosis and management of essential thrombocythemia. Seminars in thrombosis and hemostasis. 2006;32:430–436. - PubMed
-
- Pearson TC. Diagnosis and classification of erythrocytoses and thrombocytoses. Baillieres Clinical Haematology. 1998;11:695–720. - PubMed
-
- Murphy S. Diagnostic criteria and prognosis in polycythemia vera and essential thrombocythemia. Semin Hematol. 1999;36:9–13. - PubMed
-
- Finazzi G, Harrison C. Essential thrombocythemia. Seminars in hematology. 2005;42:230–238. - PubMed
-
- Weinberg RS. In vitro erythropoiesis in polycythemia vera and other myeloproliferative disorders. Seminars in hematology. 1997;34:64–69. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
