

In vitro and in vivo demonstration of risperidone implants in mice
- PMID: 17765477
- PMCID: PMC2561216
- DOI: 10.1016/j.schres.2007.08.003
In vitro and in vivo demonstration of risperidone implants in mice
Abstract
Background: Non-adherence with medication is a critical limitation in current long-term treatment of schizophrenia and a primary factor in poor quality-of-life outcomes. However, few treatments have addressed this shortcoming using an implantable drug delivery approach. The goal of this study was to provide in vitro and in vivo proof of concept for a long-term implantable risperidone delivery system in mice.
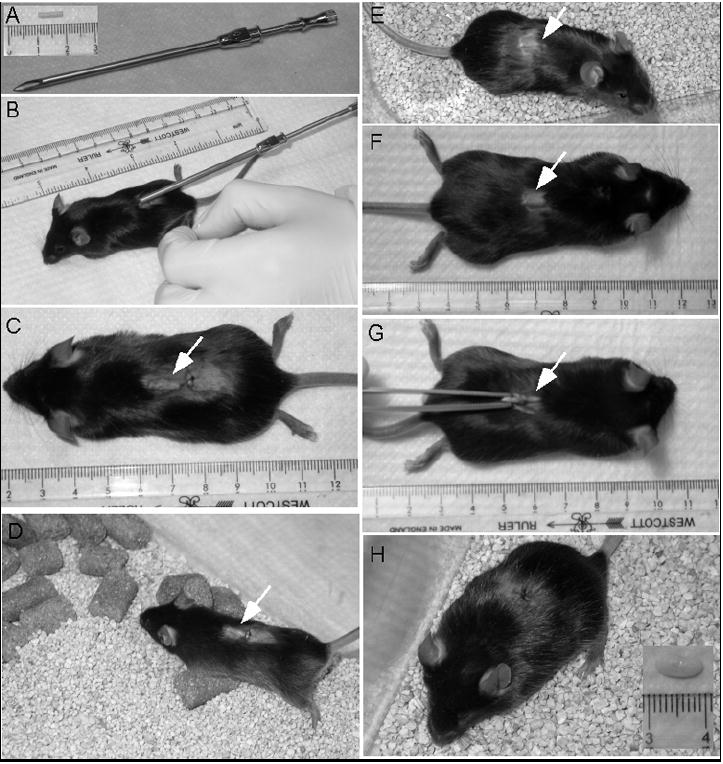
Methods: Implantable formulations of risperidone were created using the biodegradable polymer Poly Lactic co Glycolic Acid (PLGA) combined with various drug loads. Implant bioactivity was tested using in vitro release and stability studies, as well as in vivo pharmacokinetic and behavioral studies in mice.
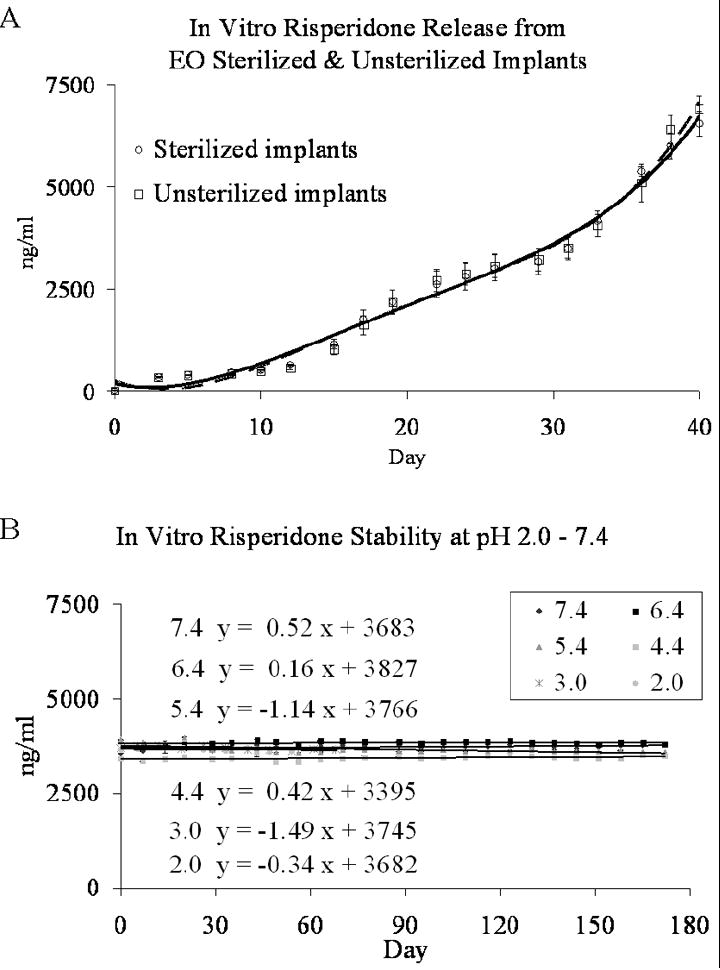
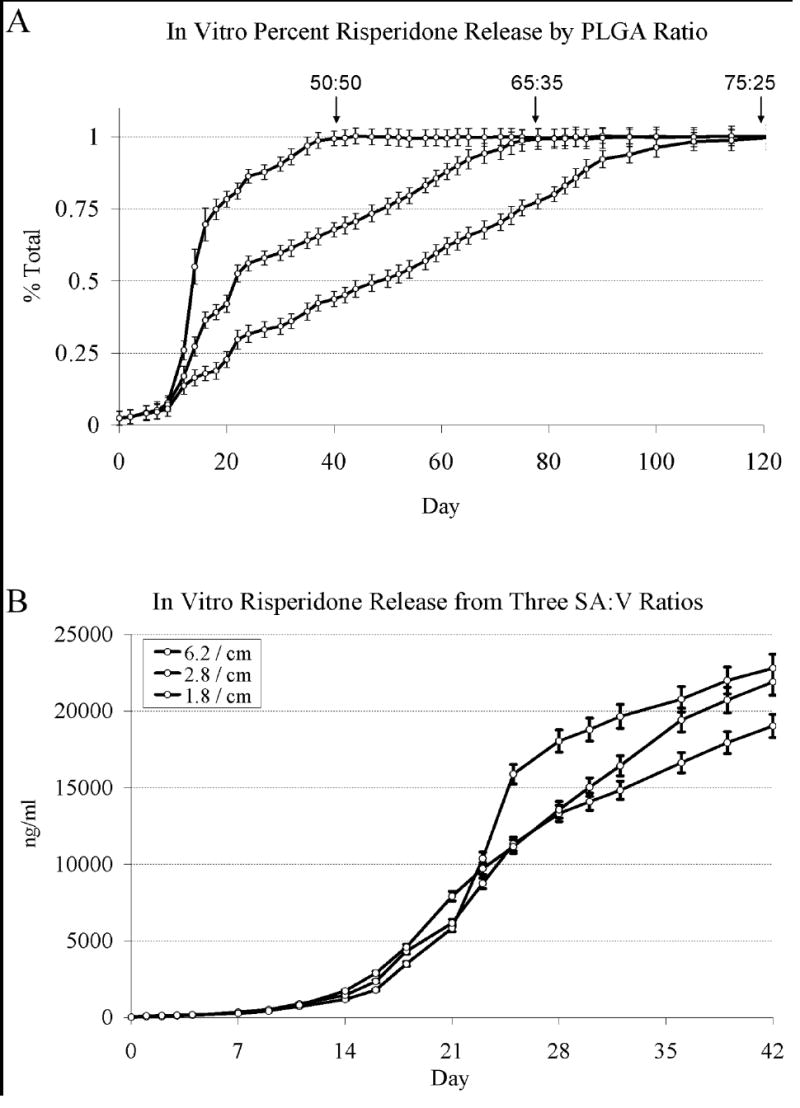
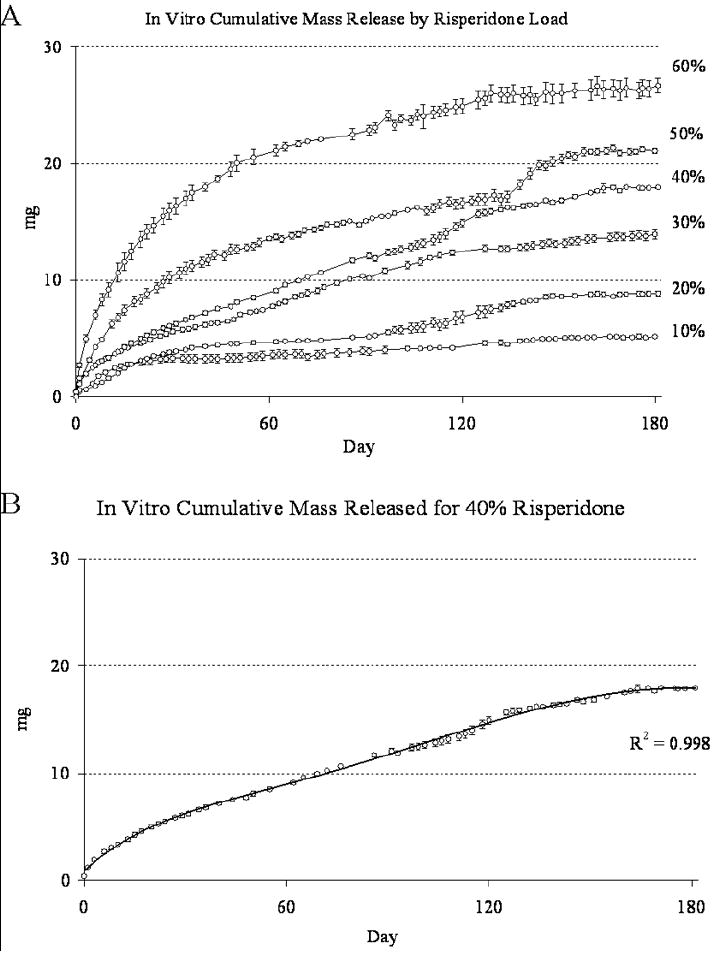
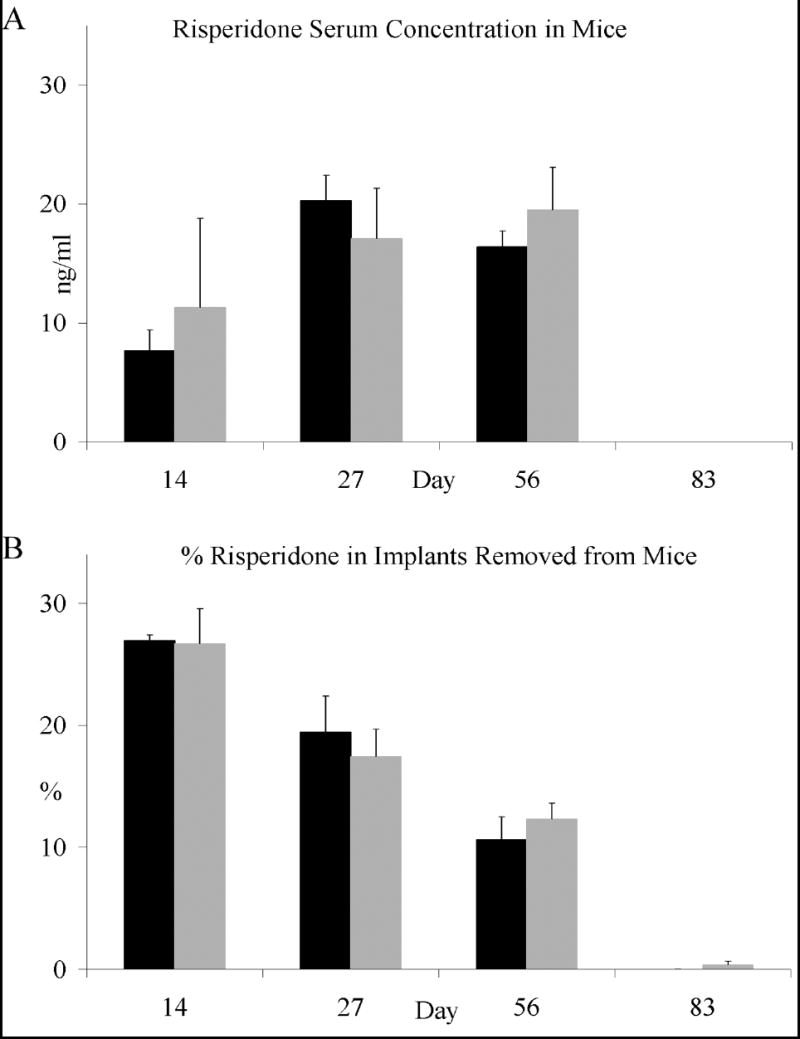
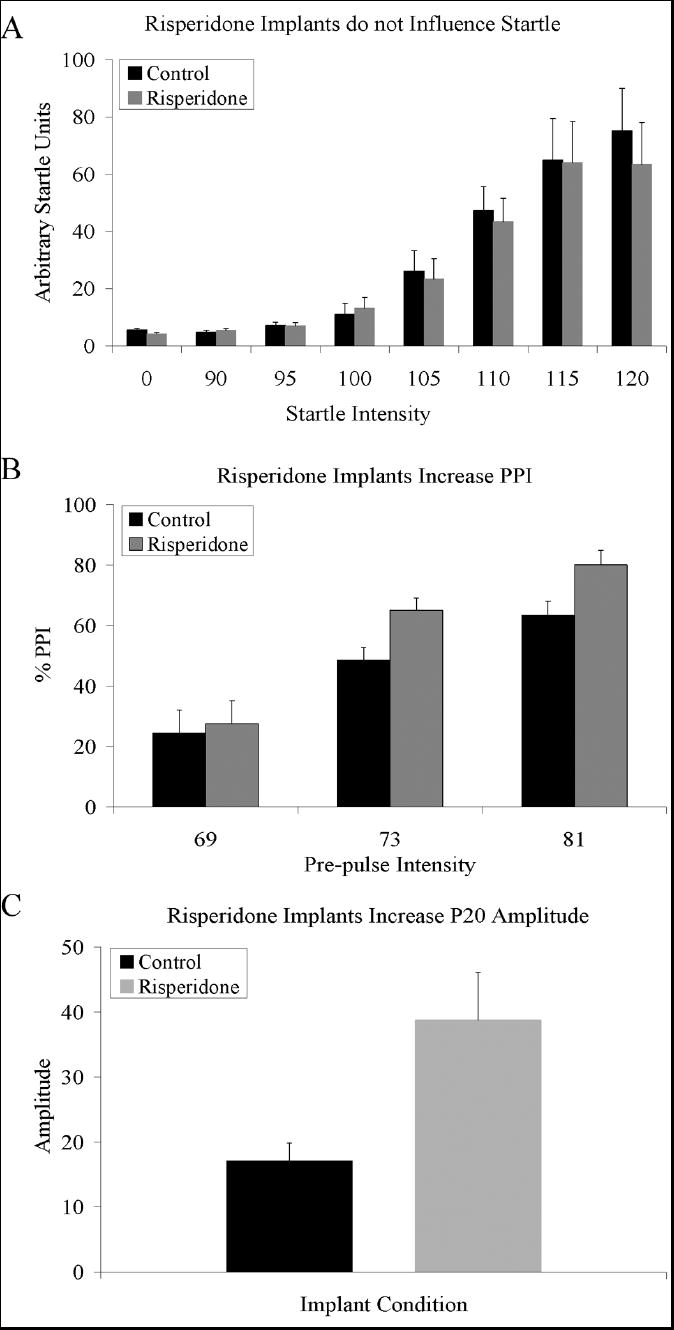
Results: The pattern of risperidone release is influenced by various parameters, including polymer composition and drug load. In vitro measures demonstrate that risperidone is stable in implants under physiological conditions. Behavioral measures demonstrate the bioactivity of risperidone implants delivering 3 mg/kg/day in mice, while pharmacokinetic analyses indicate that reversibility is maintained throughout the delivery interval.
Conclusions: The current report suggests that implantable formulations are a viable approach to providing long-term delivery of antipsychotic medications based on in vivo animal studies and pharmacokinetics. Implantable medications demonstrated here can last two months or longer while maintaining coherence and removability past full release, suggesting a potential paradigm shift in the long-term treatment of schizophrenia.
Figures
Similar articles
-
In vitro-in vivo correlations of scalable PLGA-risperidone implants for the treatment of schizophrenia.Pharm Res. 2010 Aug;27(8):1730-7. doi: 10.1007/s11095-010-0152-4. Epub 2010 Apr 27. Pharm Res. 2010. PMID: 20422263
-
Pharmacokinetic and behavioral characterization of a long-term antipsychotic delivery system in rodents and rabbits.Psychopharmacology (Berl). 2007 Feb;190(2):201-11. doi: 10.1007/s00213-006-0616-8. Epub 2006 Nov 21. Psychopharmacology (Berl). 2007. PMID: 17119931
-
Schizophrenia Treatment Based on Sustained Release of Risperidone from Poly(lactic-co-glycolic) Acid Implantable Microarray Patch.ACS Appl Mater Interfaces. 2025 Mar 19;17(11):16616-16631. doi: 10.1021/acsami.4c20010. Epub 2025 Mar 6. ACS Appl Mater Interfaces. 2025. PMID: 40048359 Free PMC article.
-
Biodegradable polymers for ocular drug delivery.Ophthalmologica. 2001 May-Jun;215(3):143-55. doi: 10.1159/000050849. Ophthalmologica. 2001. PMID: 11340382 Review.
-
Synthetic biodegradable polyesters for implantable controlled-release devices.Expert Opin Drug Deliv. 2022 Oct;19(10):1351-1364. doi: 10.1080/17425247.2022.2131768. Epub 2022 Oct 25. Expert Opin Drug Deliv. 2022. PMID: 36197839 Review.
Cited by
-
Development of novel risperidone implants using blends of polycaprolactones and in vitro in vivo correlation studies.J Adv Pharm Technol Res. 2014 Apr;5(2):84-9. doi: 10.4103/2231-4040.133431. J Adv Pharm Technol Res. 2014. PMID: 24959417 Free PMC article.
-
The role of long-acting injectable antipsychotics in schizophrenia: a critical appraisal.Ther Adv Psychopharmacol. 2014 Oct;4(5):198-219. doi: 10.1177/2045125314540297. Ther Adv Psychopharmacol. 2014. PMID: 25360245 Free PMC article. Review.
-
Poly(lactic-co-glycolic acid) devices: Production and applications for sustained protein delivery.Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2018 Sep;10(5):e1516. doi: 10.1002/wnan.1516. Epub 2018 Mar 13. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 2018. PMID: 29536634 Free PMC article. Review.
-
A method to slow down the ionization-dependent release of risperidone loaded in a thermoresponsive poly(N-acryloyl glycinamide) hydrogel.Drug Deliv Transl Res. 2017 Jun;7(3):460-464. doi: 10.1007/s13346-017-0376-5. Drug Deliv Transl Res. 2017. PMID: 28389859
-
In vitro-in vivo correlations of scalable PLGA-risperidone implants for the treatment of schizophrenia.Pharm Res. 2010 Aug;27(8):1730-7. doi: 10.1007/s11095-010-0152-4. Epub 2010 Apr 27. Pharm Res. 2010. PMID: 20422263
References
-
- Barnes TR, Curson DA. Long-term depot antipsychotics. A risk-benefit assessment. Drug Saf. 1994;10:464–479. - PubMed
-
- Bloch YMS, Strupinsky S, Altshuler A, Fennig S, Ratzoni G. Injections of depot antipsychotic medications in patients suffering from schizophrenia: do they hurt? Journal of Clinical Psychiatry. 2001;62:855–859. - PubMed
-
- Boutros N, Korzyukov O, Jansen B, Feingold A, Bell M. Sensory gating deficits during the mid-latency phase of information processing in medicated schizophrenia patients. Psychiatry Research. 2004;126:203–215. - PubMed
-
- Connolly PM, Maxwell C, Liang Y, Kahn JB, Kanes SJ, Abel T, et al. The effects of ketamine vary among inbred mouse strains and mimic schizophrenia for the P80, but not P20 or N40 auditory ERP components. Neurochem Res. 2004;29:1179–1188. - PubMed
-
- de Oliveira IM-SAdSEPERMdC-e-SEBJ. Risperidone versus haloperidol in the treatment of schizophrenia: a meta-analysis comparing their efficacy and safety. J Clin Pharm Ther. 1996;21:349–358. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
