

Pulmonary hypertension associated with sarcoidosis
- PMID: 17767746
- PMCID: PMC2072890
- DOI: 10.1186/ar2192
Pulmonary hypertension associated with sarcoidosis
Abstract
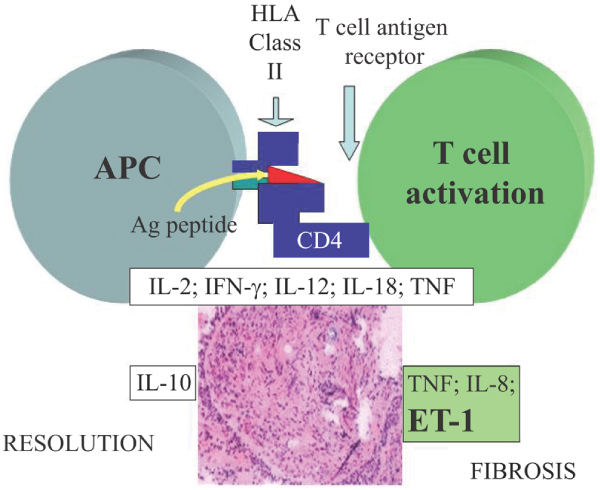
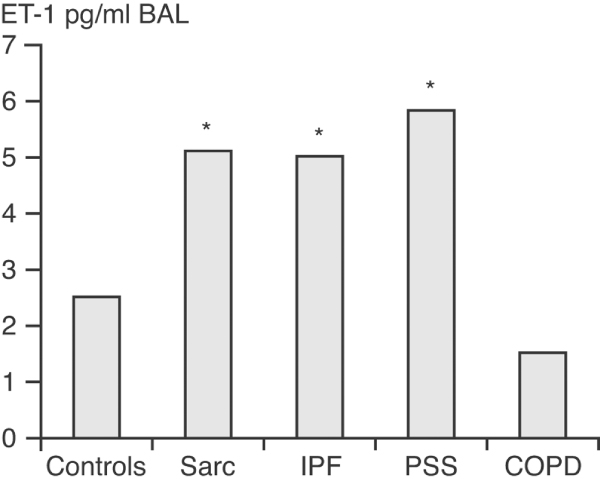
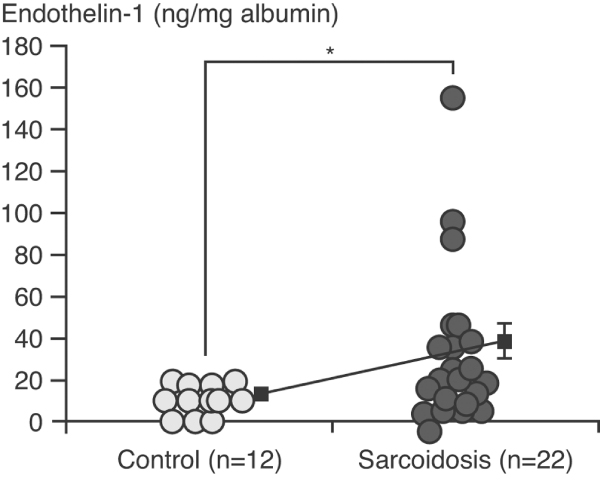
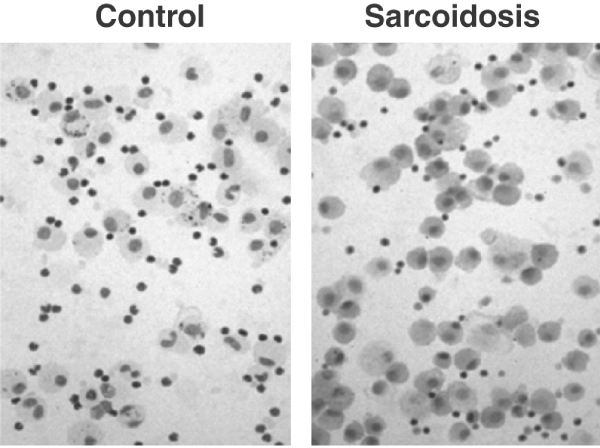
Pulmonary involvement is common in sarcoidosis, an immune-mediated inflammatory disorder that is characterized by non-caseating granulomas in tissue. Sarcoid patients with advanced pulmonary disease, especially end-stage pulmonary fibrosis, risk developing pulmonary hypertension (World Health Organization group III pulmonary hypertension secondary to hypoxic lung disease). Increased levels of endothelin (ET)-1 in plasma and bronchoalveolar lavage of some sarcoid patients suggest that ET-1 may be driving pulmonary fibrosis and sarcoidosis-associated pulmonary hypertension. Although a relationship between raised levels of ET-1 and clinical phenotype is yet to be identified, early evidence from studies of ET-1 blockade with drugs such as bosentan is encouraging. Such therapy possibly could be combined with standard anti-inflammatory agents to improve outcome.
Figures
Similar articles
-
Sarcoidosis-associated pulmonary hypertension: a role for endothelin receptor antagonists?Ther Adv Respir Dis. 2009 Jun;3(3):99-101. doi: 10.1177/1753465809341650. Epub 2009 Jul 28. Ther Adv Respir Dis. 2009. PMID: 19638368
-
Management of end-stage sarcoidosis: pulmonary hypertension and lung transplantation.Eur Respir J. 2012 Jun;39(6):1520-33. doi: 10.1183/09031936.00175511. Epub 2012 Jan 12. Eur Respir J. 2012. PMID: 22241743 Review.
-
Pulmonary fibrosis in sarcoidosis. Clinical features and outcomes.Ann Am Thorac Soc. 2013 Aug;10(4):362-70. doi: 10.1513/AnnalsATS.201303-069FR. Ann Am Thorac Soc. 2013. PMID: 23952859 Review.
-
Sarcoidosis-associated pulmonary hypertension: assessment and management.Semin Respir Crit Care Med. 2010 Aug;31(4):494-500. doi: 10.1055/s-0030-1262217. Epub 2010 Jul 27. Semin Respir Crit Care Med. 2010. PMID: 20665399 Review.
-
Pulmonary hypertension complicating sarcoidosis.Intern Med J. 2008 Jul;38(7):613-4; author reply 614. doi: 10.1111/j.1445-5994.2008.01682.x. Intern Med J. 2008. PMID: 18715311 No abstract available.
Cited by
-
Right Ventricular Abnormalities on Cardiovascular Magnetic Resonance Imaging in Patients With Sarcoidosis.JACC Cardiovasc Imaging. 2020 Jun;13(6):1395-1405. doi: 10.1016/j.jcmg.2019.12.011. Epub 2020 Jan 15. JACC Cardiovasc Imaging. 2020. PMID: 31954639 Free PMC article.
-
Sarcoidosis-associated pulmonary hypertension and lung transplantation for sarcoidosis.Semin Respir Crit Care Med. 2014 Jun;35(3):362-71. doi: 10.1055/s-0034-1376863. Epub 2014 Jul 9. Semin Respir Crit Care Med. 2014. PMID: 25007088 Free PMC article. Review.
-
Pulmonary hypertension caused by sarcoidosis.Clin Chest Med. 2008 Sep;29(3):549-63, x. doi: 10.1016/j.ccm.2008.03.010. Clin Chest Med. 2008. PMID: 18539244 Free PMC article. Review.
-
An inhibitory effect of tumor necrosis factor-alpha antagonist to gene expression in monocrotaline-induced pulmonary hypertensive rats model.Korean J Pediatr. 2013 Mar;56(3):116-24. doi: 10.3345/kjp.2013.56.3.116. Epub 2013 Mar 18. Korean J Pediatr. 2013. PMID: 23559973 Free PMC article.
-
Fibrotic Pulmonary Sarcoidosis-From Pathogenesis to Management.J Clin Med. 2025 Mar 30;14(7):2381. doi: 10.3390/jcm14072381. J Clin Med. 2025. PMID: 40217830 Free PMC article. Review.
References
-
- Bihl MP, Laule-Kilian K, Bubendorf L, Rutherford RM, Baty F, Kehren J, Eryuksel E, Staedtler F, Yang JQ, Goulet S, et al. Progressive pulmonary sarcoidosis: a fibroproliferative process potentially triggered by EGR-1 and IL-6. Sarcoidosis Vasc Diffuse Lung Dis. 2006;23:38–50. - PubMed
-
- Eishi Y, Suga M, Ishige I, Kobayashi D, Yamada T, Takemura T, Takizawa T, Koike M, Kudoh S, Costabel U, et al. Quantitative analysis of mycobacterial and propionibacterial DNA in lymph nodes of Japanese and European patients with sarcoidosis. J Clin Microbiol. 2002;40:198–204. doi: 10.1128/JCM.40.1.198-204.2002. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
