

Acute graft versus host disease
- PMID: 17784964
- PMCID: PMC2018687
- DOI: 10.1186/1750-1172-2-35
Acute graft versus host disease
Abstract
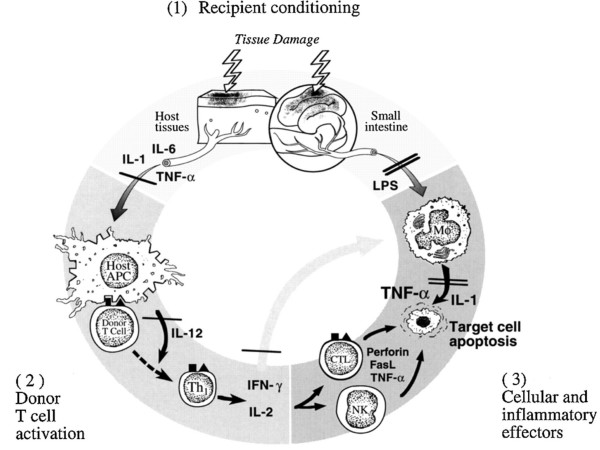
Acute graft-versus-host disease (GVHD) occurs after allogeneic hematopoietic stem cell transplant and is a reaction of donor immune cells against host tissues. Activated donor T cells damage host epithelial cells after an inflammatory cascade that begins with the preparative regimen. About 35%-50% of hematopoietic stem cell transplant (HSCT) recipients will develop acute GVHD. The exact risk is dependent on the stem cell source, age of the patient, conditioning, and GVHD prophylaxis used. Given the number of transplants performed, we can expect about 5500 patients/year to develop acute GVHD. Patients can have involvement of three organs: skin (rash/dermatitis), liver (hepatitis/jaundice), and gastrointestinal tract (abdominal pain/diarrhea). One or more organs may be involved. GVHD is a clinical diagnosis that may be supported with appropriate biopsies. The reason to pursue a tissue biopsy is to help differentiate from other diagnoses which may mimic GVHD, such as viral infection (hepatitis, colitis) or drug reaction (causing skin rash). Acute GVHD is staged and graded (grade 0-IV) by the number and extent of organ involvement. Patients with grade III/IV acute GVHD tend to have a poor outcome. Generally the patient is treated by optimizing their immunosuppression and adding methylprednisolone. About 50% of patients will have a solid response to methylprednisolone. If patients progress after 3 days or are not improved after 7 days, they will get salvage (second-line) immunosuppressive therapy for which there is currently no standard-of-care. Well-organized clinical trials are imperative to better define second-line therapies for this disease. Additional management issues are attention to wound infections in skin GVHD and fluid/nutrition management in gastrointestinal GVHD. About 50% of patients with acute GVHD will eventually have manifestations of chronic GVHD.
Figures
References
-
- Przepiorka D, Weisdorf D, Martin P, Klingemann HG, Beatty P, Hows J, Thomas ED. 1994 Consensus Conference on Acute GVHD Grading. Bone Marrow Transplant. 1995;15:825–828. - PubMed
-
- Martin PJ, McDonald GB, Sanders JE, Anasetti C, Appelbaum FR, Deeg HJ, Nash RA, Petersdorf EW, Hansen JA, Storb R. Increasingly frequent diagnosis of acute gastrointestinal graft-versus-host disease after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2004;10:320–327. doi: 10.1016/j.bbmt.2003.12.304. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
