

A systematic review of cooling for neuroprotection in neonates with hypoxic ischemic encephalopathy - are we there yet?
- PMID: 17784966
- PMCID: PMC2031882
- DOI: 10.1186/1471-2431-7-30
A systematic review of cooling for neuroprotection in neonates with hypoxic ischemic encephalopathy - are we there yet?
Abstract
Background: The objective of this study was to systematically review randomized trials assessing therapeutic hypothermia as a treatment for term neonates with hypoxic ischemic encephalopathy.
Methods: The Cochrane Central Register of Controlled Trials, MEDLINE, EMBASE, CINAHL databases, reference lists of identified studies, and proceedings of the Pediatric Academic Societies were searched in July 2006. Randomized trials assessing the effect of therapeutic hypothermia by either selective head cooling or whole body cooling in term neonates were eligible for inclusion in the meta-analysis. The primary outcome was death or neurodevelopmental disability at >or= 18 months.
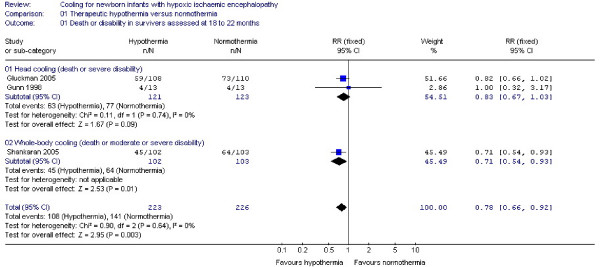
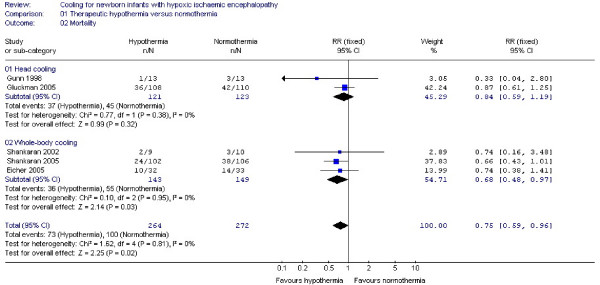
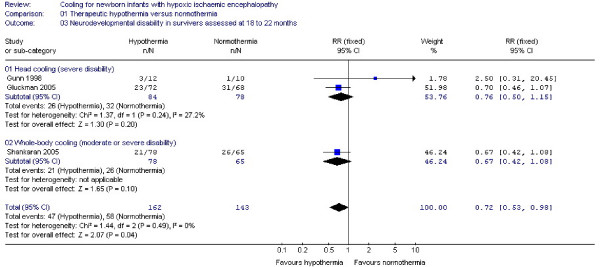
Results: Five trials involving 552 neonates were included in the analysis. Cooling techniques and the definition and severity of neurodevelopmental disability differed between studies. Overall, there is evidence of a significant effect of therapeutic hypothermia on the primary composite outcome of death or disability (RR: 0.78, 95% CI: 0.66, 0.92, NNT: 8, 95% CI: 5, 20) as well as on the single outcomes of mortality (RR: 0.75, 95% CI: 0.59, 0.96) and neurodevelopmental disability at 18 to 22 months (RR: 0.72, 95% CI: 0.53, 0.98). Adverse effects include benign sinus bradycardia (RR: 7.42, 95% CI: 2.52, 21.87) and thrombocytopenia (RR: 1.47, 95% CI: 1.07, 2.03, NNH: 8) without deleterious consequences.
Conclusion: In general, therapeutic hypothermia seems to have a beneficial effect on the outcome of term neonates with moderate to severe hypoxic ischemic encephalopathy. Despite the methodological differences between trials, wide confidence intervals, and the lack of follow-up data beyond the second year of life, the consistency of the results is encouraging. Further research is necessary to minimize the uncertainty regarding efficacy and safety of any specific technique of cooling for any specific population.
Figures
Similar articles
-
Cooling for newborns with hypoxic ischaemic encephalopathy.Cochrane Database Syst Rev. 2007 Oct 17;(4):CD003311. doi: 10.1002/14651858.CD003311.pub2. Cochrane Database Syst Rev. 2007. Update in: Cochrane Database Syst Rev. 2013 Jan 31;(1):CD003311. doi: 10.1002/14651858.CD003311.pub3. PMID: 17943788 Updated.
-
Xenon as an adjuvant to therapeutic hypothermia in near-term and term newborns with hypoxic-ischaemic encephalopathy.Cochrane Database Syst Rev. 2018 Aug 20;8(8):CD012753. doi: 10.1002/14651858.CD012753.pub2. Cochrane Database Syst Rev. 2018. PMID: 30123976 Free PMC article.
-
Interventions for infantile haemangiomas of the skin.Cochrane Database Syst Rev. 2018 Apr 18;4(4):CD006545. doi: 10.1002/14651858.CD006545.pub3. Cochrane Database Syst Rev. 2018. PMID: 29667726 Free PMC article.
-
Cooling for newborns with hypoxic ischaemic encephalopathy.Cochrane Database Syst Rev. 2003;(4):CD003311. doi: 10.1002/14651858.CD003311. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2007 Oct 17;(4):CD003311. doi: 10.1002/14651858.CD003311.pub2. PMID: 14583966 Updated.
-
Different corticosteroids and regimens for accelerating fetal lung maturation for babies at risk of preterm birth.Cochrane Database Syst Rev. 2022 Aug 9;8(8):CD006764. doi: 10.1002/14651858.CD006764.pub4. Cochrane Database Syst Rev. 2022. PMID: 35943347 Free PMC article.
Cited by
-
Cooling for newborns with hypoxic ischaemic encephalopathy.Cochrane Database Syst Rev. 2013 Jan 31;2013(1):CD003311. doi: 10.1002/14651858.CD003311.pub3. Cochrane Database Syst Rev. 2013. PMID: 23440789 Free PMC article.
-
Lessons learned during implementation of therapeutic hypothermia for neonatal hypoxic ischemic encephalopathy in a regional transport program in Ontario.Paediatr Child Health. 2011 Mar;16(3):153-6. doi: 10.1093/pch/16.3.153. Paediatr Child Health. 2011. PMID: 22379379 Free PMC article.
-
Protocol for a Magnetic Resonance Imaging (MRI) Study of Participants in the Fever Randomized Controlled Trial: Does fever control prevent brain injury in malaria?medRxiv [Preprint]. 2023 Nov 10:2023.11.10.23298374. doi: 10.1101/2023.11.10.23298374. medRxiv. 2023. PMID: 37986869 Free PMC article. Preprint.
-
Aggressive antipyretics in central nervous system malaria: Study protocol of a randomized-controlled trial assessing antipyretic efficacy and parasite clearance effects (Malaria FEVER study).PLoS One. 2022 Oct 7;17(10):e0268414. doi: 10.1371/journal.pone.0268414. eCollection 2022. PLoS One. 2022. PMID: 36206262 Free PMC article.
-
Effect of hypothermia on motor function of adult rats after neonatal hyperthermic hypoxic-ischemic brain insult.Eur J Appl Physiol. 2010 May;109(1):35-9. doi: 10.1007/s00421-009-1156-9. Epub 2009 Aug 14. Eur J Appl Physiol. 2010. PMID: 19685071
References
-
- Vannucci RC. Current and potentially new management strategies for perinatal hypoxic-ischemic encephalopathy. Pediatrics. 1990;85:961–968. - PubMed
-
- Jacobs S, Hunt R, Tarnow-Mordi W, Inder T, Davis P. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst Rev. 2003:CD003311. - PubMed
-
- Cordey R. Resuscitation of the newborn in white asphyxia by means of hypothermia alone or combined with intra-arterial transfusion of oxygenated blood. Bull Fed Soc Gynecol Obstet Lang Fr. 1961;13:507–509. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
