

Impact of antiretroviral therapy on the incidence of tuberculosis: the Brazilian experience, 1995-2001
- PMID: 17786198
- PMCID: PMC1952142
- DOI: 10.1371/journal.pone.0000826
Impact of antiretroviral therapy on the incidence of tuberculosis: the Brazilian experience, 1995-2001
Abstract
Background: The human immunodeficiency virus (HIV) fuels tuberculosis (TB) epidemics. In controlled clinical trials, antiretroviral therapy (ART) reduces TB incidence in HIV-infected patients. In this study we determine if, under programmatic conditions, Brazil's policy of universal ART access has impacted TB incidence among HIV-infected patients.
Methods: We abstracted clinical information from records of HIV-infected patients managed in the public sector in 11 Brazilian states between 1/1/1995 and 12/31/2001. Case ascertainment (TB and HIV) utilized guidelines (with added stringency) published by Brazil's Ministry of Health. We determined TB incidence and hazards ratio (HR) for ART-naïve and ART-treated [including highly active ART (HAART)] patients employing Cox proportional hazards analysis.
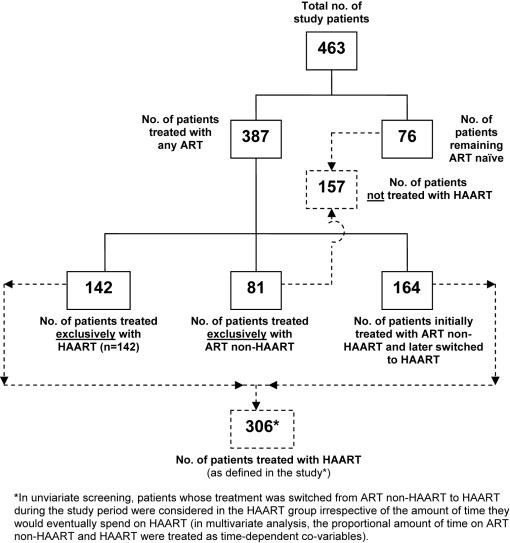
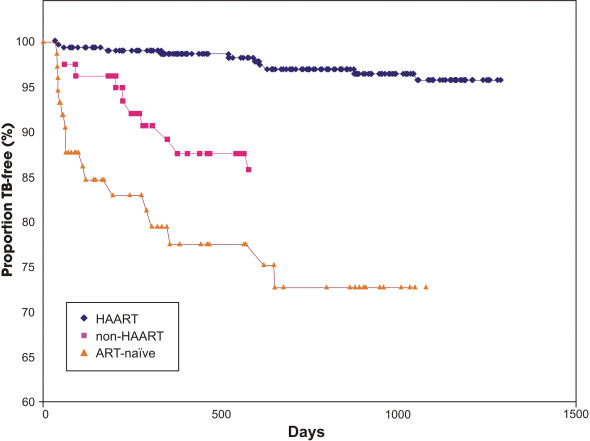
Results: Information from 463 HIV-infected patients met study criteria. The median age of the study population was 34 years, 70% were male, and mean follow-up to primary endpoints--TB, death, and last clinic visit--was 330, 1059, and 1125 days, respectively. Of the 463 patients, 76 (16%) remained ART-naïve. Of the patients who never received HAART (n = 157) 81 were treated with ART non-HAART. Of the patients who received any ART (n = 387), 306 were treated with HAART (includes those patients who later switched from ART non-HAART to HAART). Tuberculosis developed in 39/463 (8%) patients. Compared to HAART- and ART non-HAART-treated patient groups, TB incidence was 10- (p<0.001) and 2.5-fold (p = 0.03) higher in ART-naïve patients, respectively. The median baseline absolute CD4+ T-lymphocyte count for patients who developed TB was not significantly different from that of patients who remained TB free. In multivariate analysis, the incidence of TB was statistically significantly lower in HAART-treated [HR 0.2; 95% (CI 0.1, 0.6); p<0.01] compared to ART naïve patients. A baseline CD4+ T-lymphocyte count <200 cells/mm(3) [HR 2.5; (95% CI 1.2, 5.4); p<0.01], prior hospitalization [HR 4.2; (95% CI 2.0, 8.8); p<0.001], prior incarceration [HR 4.1; 95% CI 1.6, 10.3); p<0.01], and a positive tuberculin skin test [HR 3.1; (95% CI 1.1, 9.0); p = 0.04] were independently and positively associated with incident TB.
Conclusion: In this population-based study we demonstrate an 80% reduction in incident TB, under programmatic conditions, in HAART-treated HIV-infected patients compared to ART-naïve patients.
Conflict of interest statement
Figures
References
-
- Hopewell PC, Chaisson RE. Tuberculosis and human immunodeficiency virus Infection. In: Reichman LB, Hershfield ES, editors. Tuberculosis, a comprehensive approach, 6th ed. New York: Marcel Dekker, Inc; 2000. pp. 525–552.
-
- Grant AD, Djomand G, De Cock KM. Natural history and spectrum of disease in adults with HIV/AIDS in Africa. AIDS. 1997;11(suppl. B):S43–S54. - PubMed
-
- Corbett EL, Churchyard GJ, Charalambos S, Samb B, Moloi V, et al. Morbidity and mortality in South Africa gold miners: impact of untreated HIV infection. Clin Infect Dis. 2002;34:1251–1258. - PubMed
-
- Nunn P, Brindle R, Carpenter L. Cohort study on human immunodeficiency virus infection in patients with tuberculosis in Nairobi, Kenya. Am J Resp Crit Care Med. 1992;146:849–854. - PubMed
-
- Bucher HC, Griffith LE, Guyatt GH, Sudre P, Naef M, et al. Isoniazid prophylaxis for tuberculosis in HIV infection: a meta-analysis of randomized controlled trials. AIDS. 1999;13:501–507. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
