

The tell-tale heart: population-based surveillance reveals an association of rofecoxib and celecoxib with myocardial infarction
- PMID: 17786211
- PMCID: PMC1950690
- DOI: 10.1371/journal.pone.0000840
The tell-tale heart: population-based surveillance reveals an association of rofecoxib and celecoxib with myocardial infarction
Abstract
Background: COX-2 selective inhibitors are associated with myocardial infarction (MI). We sought to determine whether population health monitoring would have revealed the effect of COX-2 inhibitors on population-level patterns of MI.
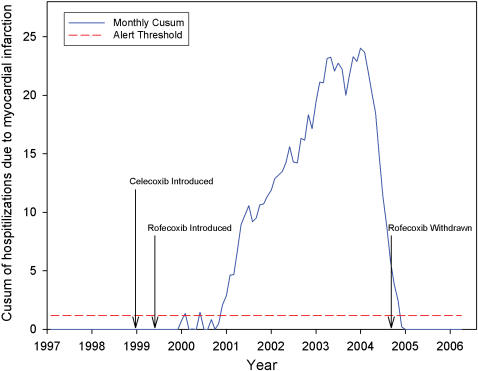
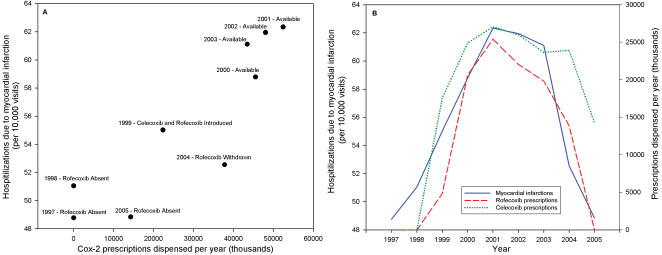
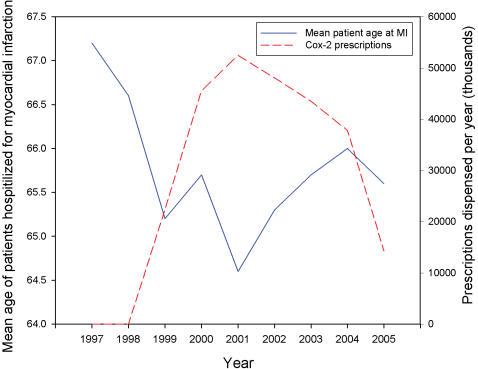
Methodology/principal findings: We conducted a retrospective study of inpatients at two Boston hospitals, from January 1997 to March 2006. There was a population-level rise in the rate of MI that reached 52.0 MI-related hospitalizations per 100,000 (a two standard deviation exceedence) in January of 2000, eight months after the introduction of rofecoxib and one year after celecoxib. The exceedence vanished within one month of the withdrawal of rofecoxib. Trends in inpatient stay due to MI were tightly coupled to the rise and fall of prescriptions of COX-2 inhibitors, with an 18.5% increase in inpatient stays for MI when both rofecoxib and celecoxib were on the market (P<0.001). For every million prescriptions of rofecoxib and celecoxib, there was a 0.5% increase in MI (95%CI 0.1 to 0.9) explaining 50.3% of the deviance in yearly variation of MI-related hospitalizations. There was a negative association between mean age at MI and volume of prescriptions for celecoxib and rofecoxib (Spearman correlation, -0.67, P<0.05).
Conclusions/significance: The strong relationship between prescribing and outcome time series supports a population-level impact of COX-2 inhibitors on MI incidence. Further, mean age at MI appears to have been lowered by use of these medications. Use of a population monitoring approach as an adjunct to pharmacovigilence methods might have helped confirm the suspected association, providing earlier support for the market withdrawal of rofecoxib.
Conflict of interest statement
Figures
References
-
- Mortality from coronary heart disease and acute myocardial infarction–United States, 1998. MMWR Morb Mortal Wkly Rep. 2001;50:90–93. - PubMed
-
- American Heart Association. Dallas, Texas: 2005. Heart Disease and Stroke Statistics-2005 Update.
-
- Willich SN, Lewis M, Lowel H, Arntz HR, Schubert F, et al. Physical exertion as a trigger of acute myocardial infarction. Triggers and Mechanisms of Myocardial Infarction Study Group. N Engl J Med. 1993;329:1684–1690. - PubMed
-
- Rosenberg L, Palmer JR, Shapiro S. Decline in the risk of myocardial infarction among women who stop smoking. N Engl J Med. 1990;322:213–217. - PubMed
-
- Hu FB, Stampfer MJ, Manson JE, Rimm E, Colditz GA, et al. Dietary fat intake and the risk of coronary heart disease in women. N Engl J Med. 1997;337:1491–1499. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
