

doi: 10.1172/JCI31791.
The evolving biology and treatment of prostate cancer
Affiliations
- PMID: 17786228
- PMCID: PMC1952634
- DOI: 10.1172/JCI31791
Item in Clipboard
The evolving biology and treatment of prostate cancer
J Clin Invest.
2007 Sep.
Abstract
Since the effectiveness of androgen deprivation for treatment of advanced prostate cancer was first demonstrated, prevention strategies and medical therapies for prostate cancer have been based on understanding the biologic underpinnings of the disease. Prostate cancer treatment is one of the best examples of a systematic therapeutic approach to target not only the cancer cells themselves, but the microenvironment in which they are proliferating. As the population ages and prostate cancer prevalence increases, challenges remain in the diagnosis of clinically relevant prostate cancer as well as the management of the metastatic and androgen-independent metastatic disease states.
Figures
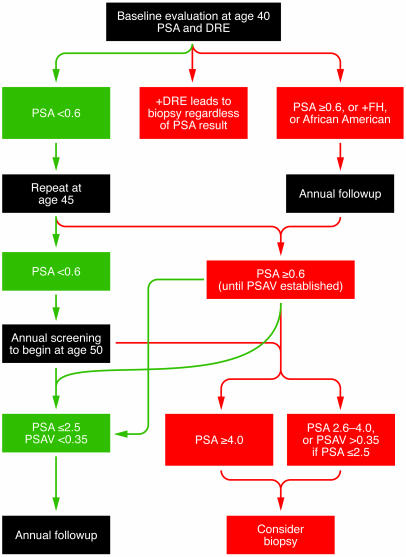
Physicians should initiate a discussion of the risks and benefits of early prostate cancer detection and offer baseline screening with DRE and PSA beginning at age 40. PSA values are shown in ng/ml. Men with PSA less than 0.6 ng/ml at age 40 should repeat screening at age 45; if PSA is less than 0.6 ng/ml at age 45, annual screening should be considered at age 50. If initial PSA at age 40 is 0.6 ng/ml or more, or if the patient has a family history of prostate cancer (+FH) or is African American, annual screening with DRE and PSA is recommended. If subsequent PSA is less than 0.6 ng/ml, the patient can repeat screening at age 45; all others should continue with annual screening. In the annual screening group, men with PSA 2.6–4.0 ng/ml, or whose PSA velocity (PSAV) exceeds 0.35 ng/ml/yr, should be considered for biopsy. Biopsy is highly recommended for any individual with PSA greater than 4.0 ng/ml and for men with positive DRE at any point in the screening process. Note that PSA velocity measurements (shown in ng/ml/yr) should be made on at least 3 consecutive specimens drawn over a period of at least 18–24 months.
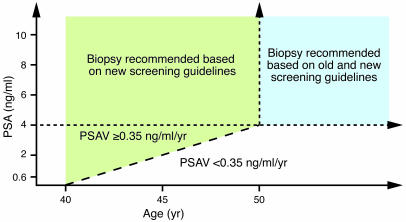
Screening that starts at age 50 still results in prostate cancers that metastasize prior to detection and are therefore incurable. The initiation of screening starting at age 40, factoring in PSA value and PSA velocity, has the goal of the detection of more clinically relevant cancers and should result in increased sensitivity of PSA as a screening test. The effect on specificity and whether this method will also result in an increase in non–clinically relevant cancers remains undetermined.
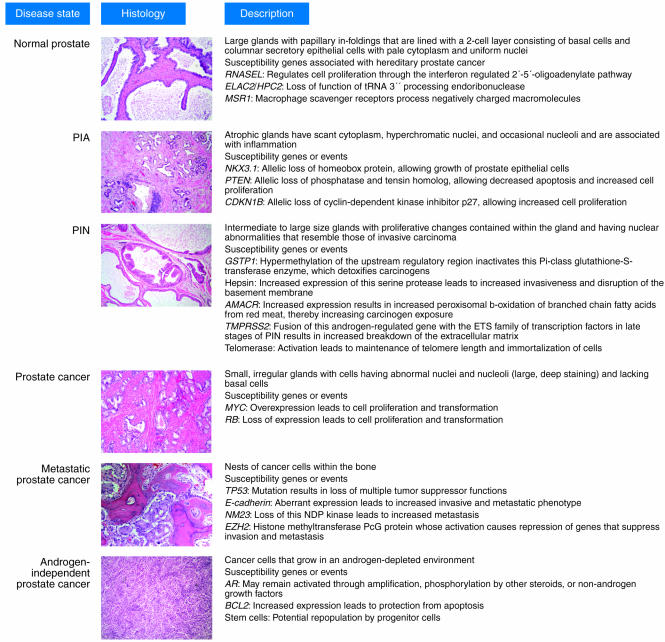
For more information, see refs. –. PIA, proliferative inflammatory atrophy; RNASEL, 2′-5′-oligoadenylate–dependent RNase L; AMACR, α-methylacyl-coenzyme A racemase; EZH2, enhancer of zeste homolog 2; PcG, polycomb group. Original magnification, ×100.
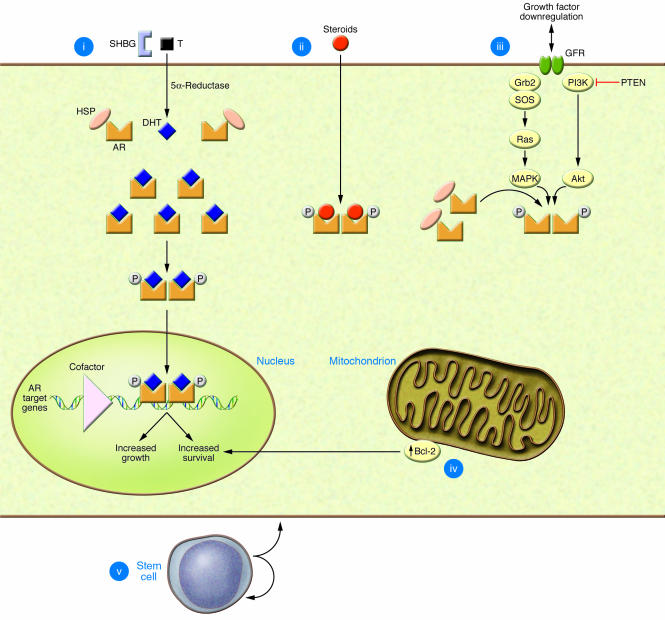
(i) Amplification. Prostate cancer cells develop the ability to utilize low levels of androgen for survival by increased sensitivity of the AR to testosterone (T), by increased local conversion of testosterone to DHT by 5α-reductase, and by increased numbers of ARs. Once DHT binds to AR, the receptor dimerizes and phosphorylates and is transported to the nucleus, where it binds to androgen-responsive elements of genes. This process is modulated by cofactors that act as coactivators and corepressors and results in increased cell proliferation and survival. (ii) Promiscuous pathway. Nonandrogenic steroid molecules normally present in the circulation, as well as antiandrogens, bind and activate the AR. (iii) Outlaw pathway. AR is activated by phosphorylation by nonhormone growth factors through their tyrosine kinase receptors. (iv) Bypass pathway. Prostate cancer cells develop the ability to survive independent of AR. The best-known bypass pathway occurs through upregulation of the molecule Bcl-2 by androgen-independent prostate cancer cells, which protects them from apoptosis. (v) Stem cell regeneration. Prostate cancer stem cells, which are not dependent on the AR for survival, continually resupply the tumor cell population. SHBG, sex hormone–binding globulin; HSP, heat shock protein; GFR, growth factor receptor; P, phosphate group; PTEN, phosphatase and tensin homolog; Grb2, growth factor receptor–bound protein–2; SOS, son of sevenless. Figure modified from Clinical Cancer Research (28).
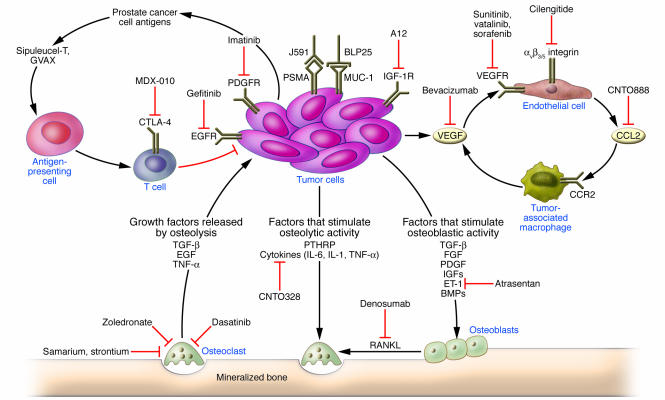
Tumor cells alter the bone microenvironment by stimulating osteoclasts parathyroid hormone–related protein (PTHRP), IL-6, IL-1, and TNF-α and by stimulating osteoblasts endothelin-1 (ET-1), FGF, PDGF, IGFs, TGF-β, and bone morphogenic proteins (BMPs). Osteolysis, in turn, releases TGF-β, TNF-α, and EGF, stimulating cancer cell proliferation. Receptor activator of NF-κB ligand (RANKL) expression by osteoblasts binds to the RANK receptor, promoting osteoclast formation and function. Therapies targeting bone metastases include those that target the prostate cancer cells themselves by inhibiting growth factor receptors or by targeting cancer cell antigens (Mucin 1 [MUC-1], BLP25 liposomal vaccine; and PSMA; J591 antibody conjugates). Alternatively, several therapies target the supporting host cells. Zoledronate, denosumab, dasatinib, CNTO328, samarium, and strontium all target osteoclast function to inhibit osteolysis. Atrasentan targets the ET-1 receptor on osteoblasts. Antiangiogenesis drugs target the endothelial cell and include bevacizumab, which targets VEGF, and cilengitide, which targets αvβ3/5 integrins. Immunotherapy approaches include inhibiting the infiltration of tumor-associated macrophages by inhibiting CCL2, prolonging T cell response by inhibiting the inhibitory receptor CTL-associated antigen–4 (CTLA-4) using the antibody ipilimumab (MDX-010), and stimulating antigen-presenting cells through vaccines such as GVAX and Sipuleucel-T. CCR2, CC chemokine receptor 2.
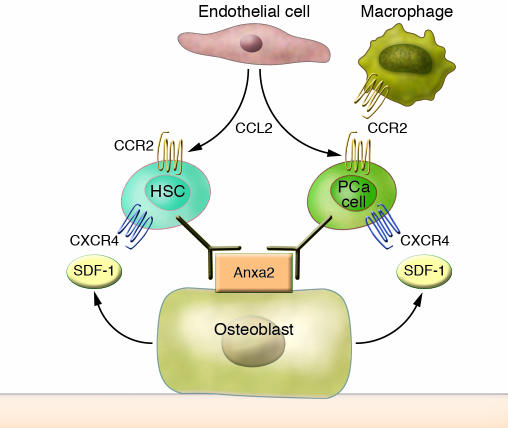
The metastatic process of prostate cancer cells (PCa cells) is functionally similar to the migrational, or homing, behavior of HSCs to the bone marrow. Numerous molecules have been implicated in regulating HSC homing, participating as both chemoattractants and regulators of cell growth. Endothelial cell–derived factors such as CCL2 act as chemoattractants and growth factors for HSCs, tumor-associated macrophages, and prostate cancer cells. Osteoblasts produce the chemokine SDF-1 (CXCL12), which further guides both HSCs and prostate cancer cells into the marrow through their expression of the CXCL12 receptor CXCR4. Both HSCs and prostate cancer cells use the cell surface protein annexin II (Anxa2) on both endothelial cells (not shown) and osteoblasts as a dock/lock mechanism into the bone microenvironment. Conceptually, prostate cancer cells act as parasites of the HSC niche by coopting HSC chemokines and attachment sites to initiate a cascade of events that result in the osteoblastic metastases observed in prostate cancer patients.
References
-
- American Cancer Society. 2007. Cancer facts and figures 2007. http://www.cancer.org/docroot/STT/content/STT_1x_Cancer_Facts__Figures_2....
-
- Scardino P.T., Weaver R., Hudson M.A. Early detection of prostate cancer. Hum. Pathol. 1992;23:211–222. - PubMed
-
- Bill-Axelson A., et al. Radical prostatectomy versus watchful waiting in early prostate cancer. . N. Engl. J. Med. 2005;352:1977–1984. - PubMed
-
- Etzioni R., et al. Overdiagnosis due to prostate-specific antigen screening: lessons from U.S. prostate cancer incidence trends. J. Natl. Cancer. Inst. 2002;94:981–990. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
