

Renal function and risk of coronary heart disease in general populations: new prospective study and systematic review
- PMID: 17803353
- PMCID: PMC1961630
- DOI: 10.1371/journal.pmed.0040270
Renal function and risk of coronary heart disease in general populations: new prospective study and systematic review
Abstract
Background: End-stage chronic kidney disease is associated with striking excesses of cardiovascular mortality, but it is uncertain to what extent renal function is related to risk of subsequent coronary heart disease (CHD) in apparently healthy adults. This study aims to quantify the association of markers of renal function with CHD risk in essentially general populations.
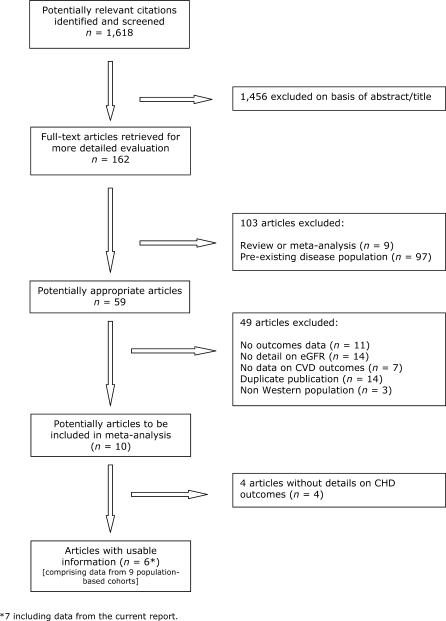
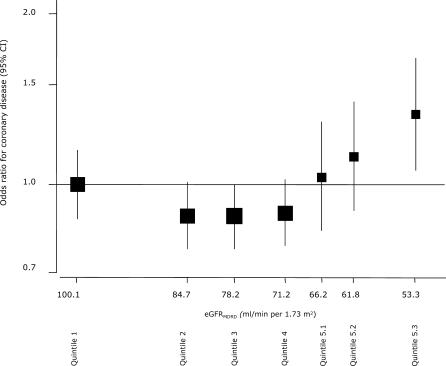
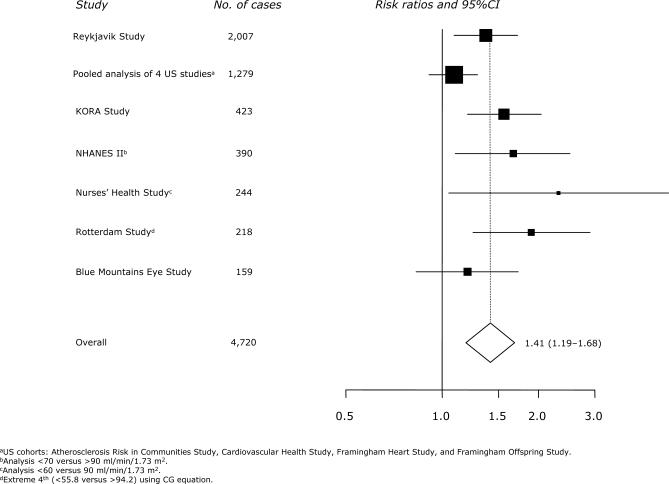
Methods and findings: Estimated glomerular filtration rate (eGFR) was calculated using standard prediction equations based on serum creatinine measurements made in 2,007 patients diagnosed with nonfatal myocardial infarction or coronary death during follow-up and in 3,869 people without CHD in the Reykjavik population-based cohort of 18,569 individuals. There were small and nonsignificant odds ratios (ORs) for CHD risk over most of the range in eGFR, except in the lowest category of the lowest fifth (corresponding to values of <60 ml/min/1.73 m2), in which the OR was 1.33 (95% confidence interval 1.01-1.75) after adjustment for several established cardiovascular risk factors. Findings from the Reykjavik study were reinforced by a meta-analysis of six previous reports (identified in electronic and other databases) involving a total of 4,720 incident CHD cases (including Reykjavik), which yielded a combined risk ratio of 1.41 (95% confidence interval 1.19-1.68) in individuals with baseline eGFR less than 60 ml/min/1.73 m2 compared with those with higher values.
Conclusions: Although there are no strong associations between lower-than-average eGFR and CHD risk in apparently healthy adults over most of the range in renal function, there may be a moderate increase in CHD risk associated with very low eGFR (i.e., renal dysfunction) in the general population. These findings could have implications for the further understanding of CHD and targeting cardioprotective interventions.
Conflict of interest statement
Figures
References
-
- Baigent C, Burbury K, Wheeler D. Premature cardiovascular disease in chronic renal failure. Lancet. 2000;356:147–152. - PubMed
-
- Sarnak MJ, Levey AS, Schoolwerth AC, Coresh J, Culleton B, et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108:2154–2169. - PubMed
-
- Anavekar NS, McMurray JJV, Velazquez EJ, Solomon SD, Kober L, et al. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N Engl J Med. 2004;351:1285–1295. - PubMed
-
- Smith GL, Lichtman JH, Bracken MB, Shlipak MG, Phillips CO, et al. Renal impairment and outcomes in heart failure: Systematic review and meta-analysis. J Amer Coll Cardiol. 2006;47:1987–1996. - PubMed
-
- Rahman M, Pressel S, Davis BR, Nwachuku C, Wright JT, Jr., et al. Cardiovascular outcomes in high-risk hypertensive patients stratified by baseline glomerular filtration rate. Ann Intern Med. 2006;144:172–180. for the ALLHAT Collaborative Research Group. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
