

Regional variability in use of a novel assessment of thoracolumbar spine fractures: United States versus international surgeons
- PMID: 17825106
- PMCID: PMC2045082
- DOI: 10.1186/1749-7922-2-24
Regional variability in use of a novel assessment of thoracolumbar spine fractures: United States versus international surgeons
Abstract
Background: Considerable variability exists in clinical approaches to thoracolumbar fractures. Controversy in evaluation and nomenclature contribute to this confusion, with significant differences found between physicians, between different specialties, and in different geographic regions. A new classification system for thoracolumbar injuries, the Thoracolumbar Injury Severity Score (TLISS), was recently described by Vaccaro. No assessment of regional differences has been described. We report regional variability in use of the TLISS system between United States and non-US surgeons.
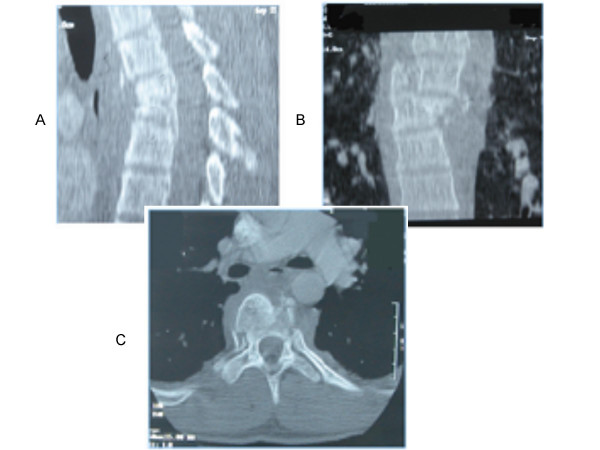
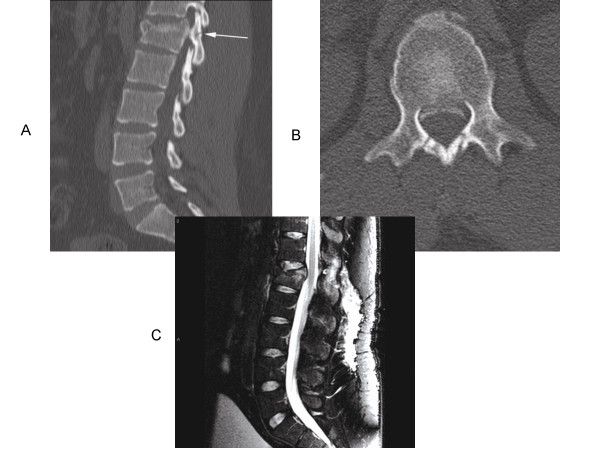
Methods: Twenty-eight spine surgeons (8 neurosurgeons and 20 orthopedic surgeons) reviewed 56 clinical thoracolumbar injury case histories, which included pertinent imaging studies. Cases were classified and scored using the TLISS system. After a three month period, the case histories were re-ordered and the physicians repeated the exercise; 22 physicians completed both surveys and were used to assess intra-rater reliability. The reliability and treatment validity of the TLISS was assessed. Surgeons were grouped into US (n = 15) and non-US (n = 13) cohorts. Inter-rater (both within and between different geographic groups) and intra-rater reliability was assessed by percent agreement, Cohen's kappa, kappa with linear weighting, and Spearman's rank-order correlation.
Conclusion: Non-US surgeons were found to have greater inter-rater reliability in injury mechanism, while agreement on neurological status and posterior ligamentous complex integrity tended to be higher among US surgeons. Inter-rater agreement on management was moderate, although it tended to be higher in US-surgeons. Inter-rater agreement between US and non-US surgeons was similar to within group inter-rater agreement for all categories. While intra-rater agreement for mechanism tended to be higher among US surgeons, intra-rater reliability for neurological status and PLC was slightly higher among non-US surgeons. Intra-rater reliability for management was substantial in both US and non-US surgeons. The TLISS incorporates generally accepted features of spinal injury assessment into a simple patient evaluation tool. The management recommendation of the treatment algorithm component of the TLISS shows good inter-rater and substantial intra-rater reliability in both non-US and US based spine surgeons. The TLISS may improve communication between health providers and may contribute to more efficient management of thoracolumbar injuries.
Figures
References
-
- Wood K, Buttermann G, Mehbod A, Garvey T, Jhanjee R, Sechriest V, Butterman G. Operative compared with nonoperative treatment of a thoracolumbar burst fracture without neurological deficit. A prospective, randomized study.[see comment][erratum appears in J Bone Joint Surg Am. 2004 Jun;86-A(6):1283] J Bone Joint Surg Am. 2003;85-A:773–781. - PubMed
-
- Vaccaro AR, Zeiller SC, Hulbert RJ, Anderson PA, Harris M, Hedlund R, Harrop J, Dvorak M, Wood K, Fehlings MG, Fisher C, Lehman RA, Jr., Anderson DG, Bono CM, Kuklo T, Oner FC. The thoracolumbar injury severity score: a proposed treatment algorithm. J Spinal Disord Tech. 2005;18:209–215. - PubMed
LinkOut - more resources
Full Text Sources
